Download to read offline












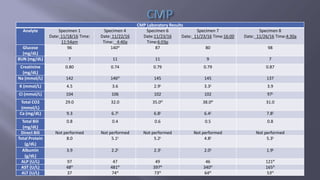
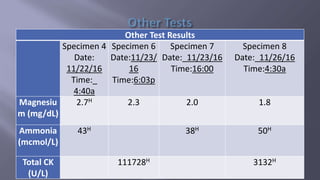







1. The patient is a 68-year-old male admitted with a subacute occlusion of his right femoral popliteal bypass graft and ischemic leg. He has a history of peripheral vascular disease, atrial fibrillation, hypertension, hyperlipidemia, and smoking. 2. His plan includes a CT/angiogram, angioplasty with stent placement, and anticoagulant therapy. During his hospital stay he undergoes the procedure and is started on medications including anticoagulants, pain medications, and nutritional support. 3. Lab results show abnormalities consistent with alcoholic liver disease including elevated liver enzymes and low albumin. The patient is discharged after 12 days with signs of revascularization and