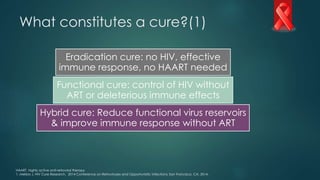
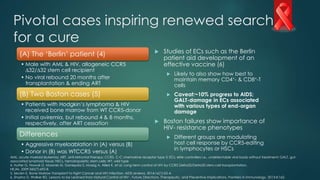
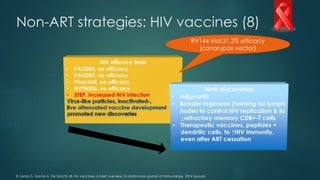
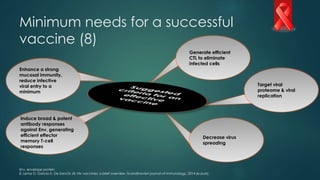
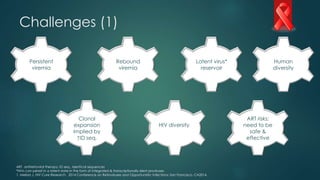
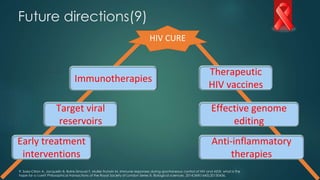
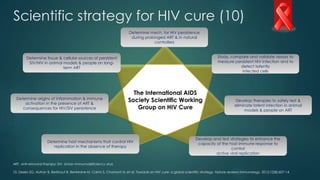
The document discusses potential strategies for curing HIV/AIDS, categorizing them into eradication, functional, and hybrid cures, alongside the role of antiretroviral therapy (ART). It highlights pivotal cases, such as the Berlin patient, that have inspired renewed research efforts for a cure and outlines non-ART strategies, including gene editing and vaccine development. Future directions focus on immunotherapies, therapeutic vaccines, and effective genome editing to target viral reservoirs and enhance the immune response.

![ART: prevention/initial treatment of
HIV+-adults & adolescents (2-3)
*CD4 counts should be done every 3 to 6 months to assess the urgency of ART initiation and the need for opportunistic infection prophylaxis. CD4 count done at baseline & repeated per tailored
management regimen; HCP, healthcare provider; mo., months; pt, patient; aPrEP candidates: when exposed to HIV e.g., through drugs /sex.
2. US Centers for Disease Control. Preexposure prophylaxis for the prevention of HIV in the United States 2014 [cited 2014 May]. : http://www.cdc.gov/hiv/pdf/guidelines/PrEPguidelines2014.pdf
3. AIDSInfo. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents: Initiating Antiretroviral Therapy in Treatment-Naive Patients: National Institute of Health; 2014
[cited 2014 May]. http://aidsinfo.nih.gov/guidelines/html/1/adult-and-adolescent-arv-guidelines/10/initiating-art-in-treatment-na%C3%AFve-patients.
PrEP candidatesa
• Truvada® used as
PrEP
• Individuals must
commit to taking
drug daily & seeing
an HCP every 3
mo. for HIV testing
& other follow-up
• Viral load &CD4-cell count*
should guide start &
continuation of ART in HIV+-
pts to reduce risk of disease
progression
• ART is recommended in
HIV+-pts. to prevent
transmission
• Pt. education: Benefit/risk
profiles & importance of
adherence
• Tailored onset/deferral of
ART may be done on a
case-by-case basis](https://image.slidesharecdn.com/hivcure16may2014-140516184421-phpapp02/85/Can-we-cure-HIV-AIDS-A-2014-progress-report-3-320.jpg)
](https://image.slidesharecdn.com/hivcure16may2014-140516184421-phpapp02/85/Can-we-cure-HIV-AIDS-A-2014-progress-report-5-320.jpg)
























![[2015] hcv direct acting antivirals [da as] stumbling](https://cdn.slidesharecdn.com/ss_thumbnails/2015hcvdirectactingantiviralsdaasstumbling-151117003903-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)













































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)
















