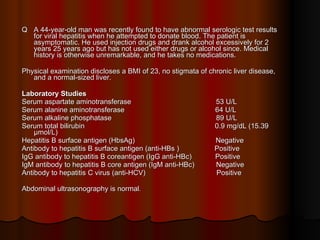
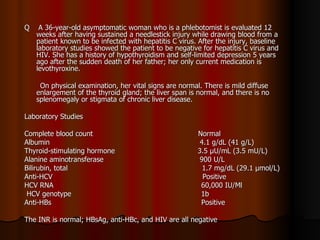
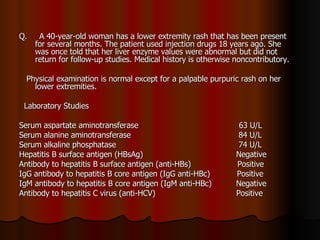
The patient has abnormal liver enzymes and tested positive for hepatitis C virus antibodies and RNA. She has a history of injection drug use 18 years ago. Her current rash and abnormal liver enzymes suggest she may have cryoglobulinemia associated with her hepatitis C infection. Measuring her serum cryoglobulins would be the most appropriate next step to evaluate for this potential extrahepatic manifestation of hepatitis C.






































































![Hepatitis B and C management (1) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hepatitisbandc1autosaved-250506091223-cc84fe1a-thumbnail.jpg?width=640&height=640&fit=bounds)




















