Downloaded 17 times










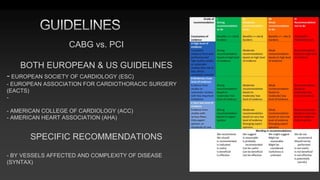
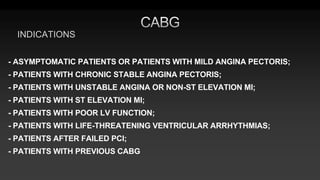





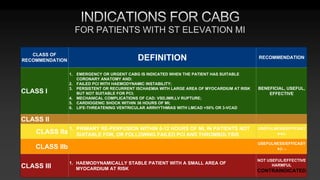







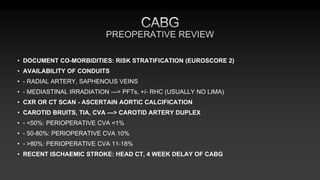



























This document discusses the history and guidelines for coronary artery bypass grafting (CABG). It provides: 1) Key events and innovations in the development of CABG, including the first successful procedures in the USSR, US, and Bulgaria. 2) Indications for CABG based on the number and location of diseased vessels and patient characteristics, as outlined in European and US guidelines. 3) Considerations for conduit choice, preoperative evaluation, and risk stratification prior to CABG. 4) An overview of how CABG differs from percutaneous coronary intervention (PCI) in treating both present and future coronary lesions due to the placement of bypass grafts in the mid coronary arteries.























































































