Downloaded 327 times

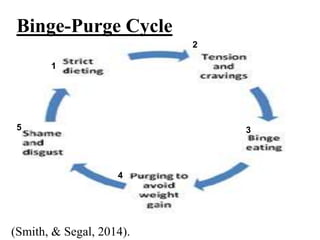




Bulimia nervosa is an eating disorder characterized by binge eating followed by purging behaviors. It commonly begins during adolescence, with various physical, psychological, and behavioral symptoms, and is associated with significant comorbid psychiatric disorders. Treatment typically involves a combination of psychotherapy, medication, and nutritional education tailored to individual needs.






















































































