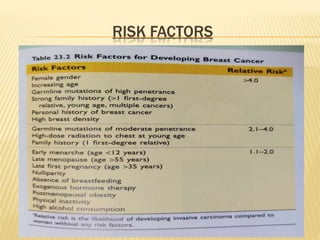
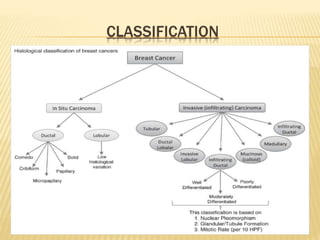
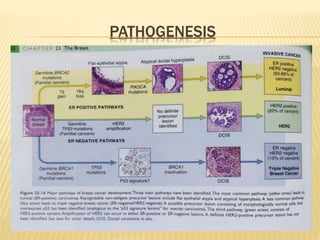
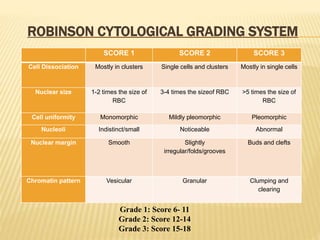
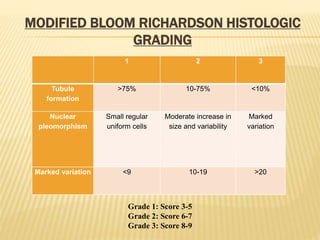
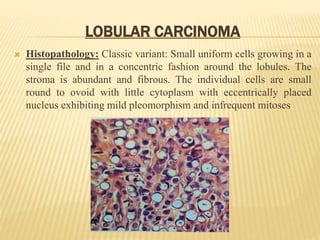
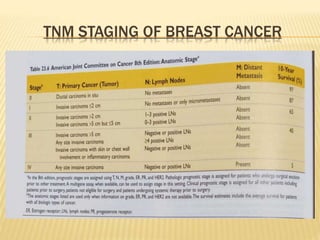
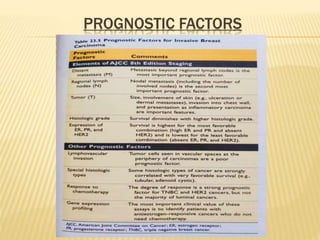
This document provides an overview of breast carcinoma. It discusses that breast cancer is the second most common cancer in females worldwide. Histological grading using the Elston-Ellis modification and cytological grading using the Robinson system are important in determining prognosis. The document outlines the structure and histology of the breast, risk factors, classification, pathogenesis, diagnostic criteria, grading systems, and types of invasive breast cancers including ductal carcinoma, tubular carcinoma, mucinous carcinoma, medullary carcinoma, and lobular carcinoma. It concludes with an overview of TNM staging and important prognostic factors for breast cancer.