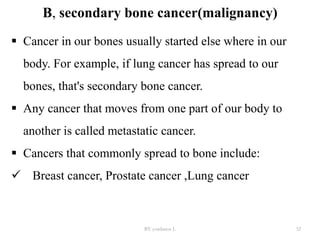
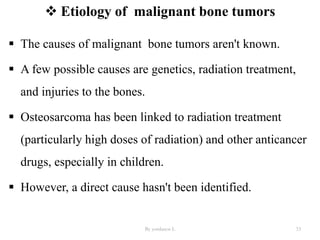
Yordanos Lemma presented on bone tumors (benign and malignant) at Salale University College of Health Science. The presentation covered:
- Types of bone tumors including the most common benign tumors like enchondroma and osteochondroma, and malignant tumors such as multiple myeloma, osteosarcoma, Ewing's sarcoma, and chondrosarcoma.
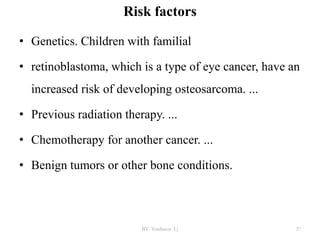
- Risk factors for bone tumors including being a child or young adult as benign tumors often affect the growing skeleton.
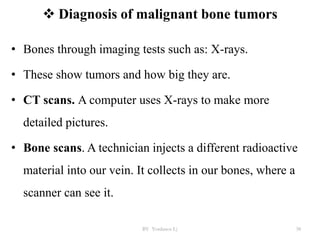
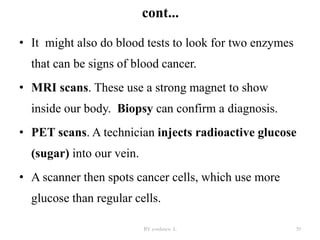
- Diagnosis involves imaging tests and biopsies to determine if a tumor is benign or malignant. Management depends on the type and severity of the tumor, ranging from observation to surgery.
![References
1.http://seer.cancer.gov/csr/1975_2008/results_single/sect_01_
table.01.pdf
2. http://www.registri-tumori.it/cms/?q=sede_osso
3. Hauben EI, Arends J, Vandenbroucke JP, et al. Multiple
primary malignancies in osteosarcoma patients. Incidence and
predictive value of osteosarcoma subtype for cancer
syndromes related with osteosarcoma.
Eur J Hum Genet. 2003;11:611–8. [PubMed] [Google Scholar]
By yordanos L 47](https://image.slidesharecdn.com/bonetumors-231002154418-13aaccd9/85/BONE-TUMORS-pptx-47-320.jpg)
![cont.…
4. Hameetman L, Bovée JV, Taminiau AH, et al.
Multiple osteochondromas: clinicopathological and
genetic spectrum and suggestions for clinical
management.
Hered Cancer Clin Pract. 2004;2:161–73. [PMC free
article] [PubMed] [Google Scholar
BY Yordanos L) 48](https://image.slidesharecdn.com/bonetumors-231002154418-13aaccd9/85/BONE-TUMORS-pptx-48-320.jpg)
























































![Immunodeficiency dis order [Repaired] FINAL.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/immunodeficiencydisorderrepairedfinal-231002162850-29300df3-thumbnail.jpg?width=640&height=640&fit=bounds)














![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












