This document summarizes evidence on blood product transfusions in critically ill children. Key points include:
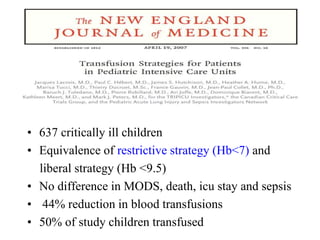
- About 50% of children in pediatric intensive care units (PICUs) receive red blood cell transfusions, though transfusion practices vary significantly between hospitals and bedside practices.
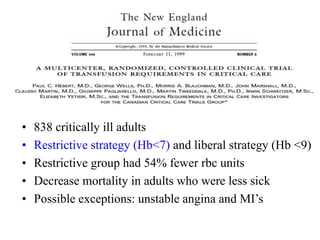
- Evidence supports a restrictive transfusion strategy (transfusing when hemoglobin is <7 g/dL) over a liberal strategy (<9.5 g/dL), as restrictive use reduces transfusions by 44% without increasing adverse outcomes.
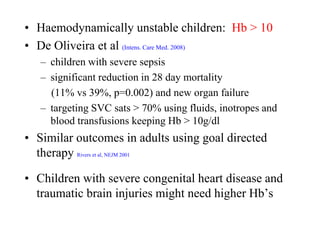
- For unstable children, such as those with severe sepsis, targeting a hemoglobin >10 g/dL through transfusions and other interventions may reduce mortality compared to lower hemoglobin levels.
-



















![CLINICAL_BLOOD_TRANSFUSION__EDITED[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalbloodtransfusionedited1-240903171619-5f7504e8-thumbnail.jpg?width=640&height=640&fit=bounds)






























![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






