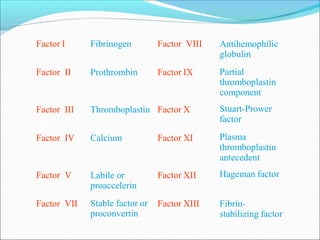
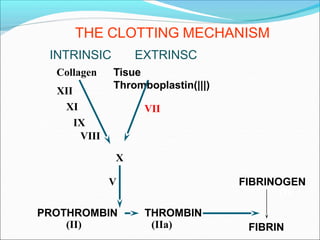
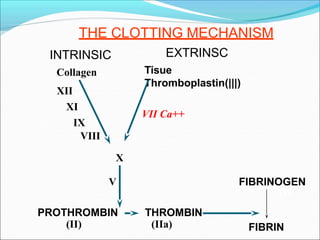
This document provides an overview of coagulation and tests used to evaluate coagulation function. It discusses how coagulation maintains hemostasis and the mechanisms involved. Factors that can cause bleeding disorders are described, including vessel defects, platelet disorders, and factor deficiencies. Key tests for evaluation of coagulation are outlined, including platelet count, bleeding time, clotting time, prothrombin time, and activated partial thromboplastin time. Specific coagulation factor deficiencies like hemophilia A, hemophilia B, and von Willebrand disease are explained. Causes of acquired bleeding disorders like anticoagulant therapy and liver disease are also summarized.















































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)

















