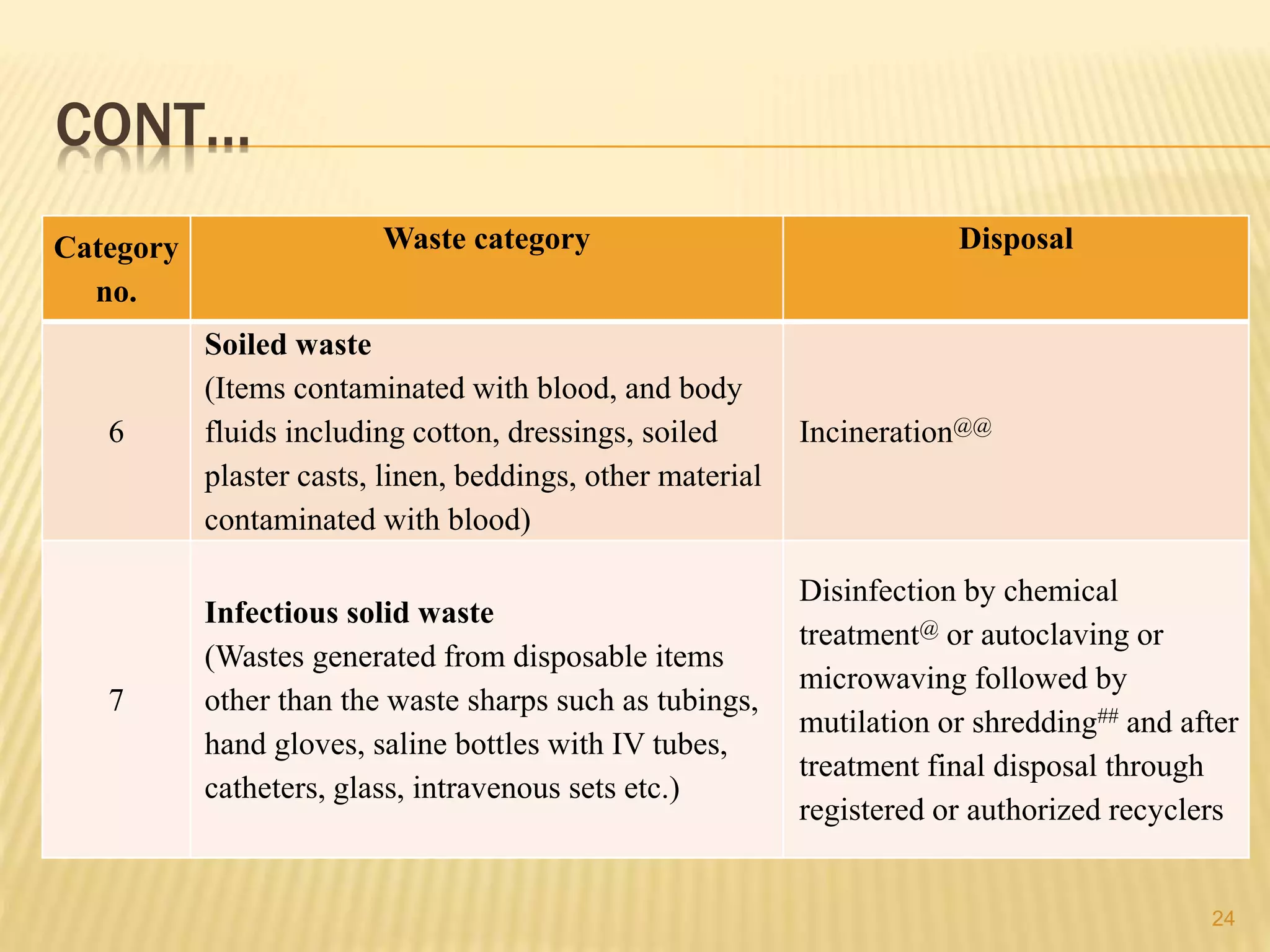
This document discusses guidelines for biomedical waste management according to the BMW rules of 1998, 2011, and 2016 in India. It defines biomedical waste and outlines the objectives of proper waste management. It describes the classification of waste into categories based on risk level and provides guidelines for segregation, treatment, and disposal of each waste category according to the color-coding system. The risks of improper waste management to health and the environment are also discussed.