The document discusses the design and mechanics of a bicycle fretsaw machine aimed at rehabilitation, operated through a cycling motion that promotes efficient pedaling technique. It details the construction, ergonomic aspects, and muscle activity involved in cycling, emphasizing the importance of proper posture and pedaling phases for effective therapy. Additionally, it outlines various applications for therapy, contraindications for cycling, and precautions to ensure safety during use.

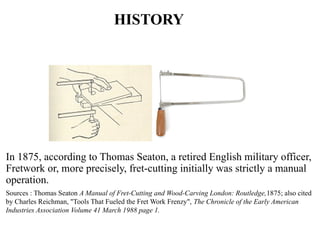
![Introduction
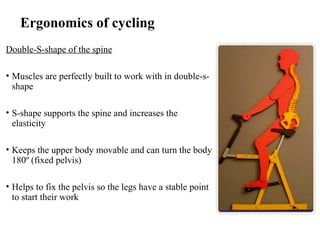
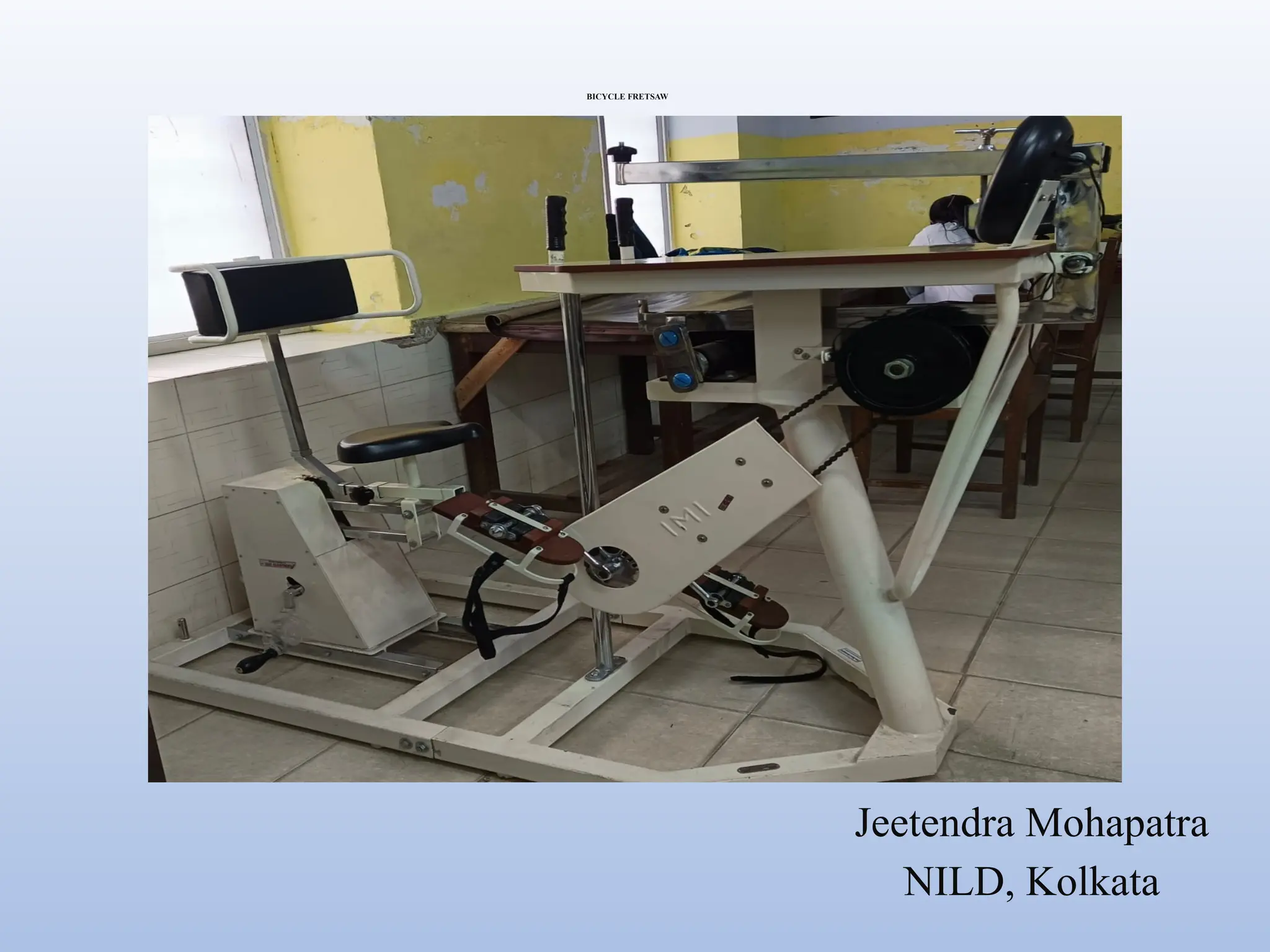
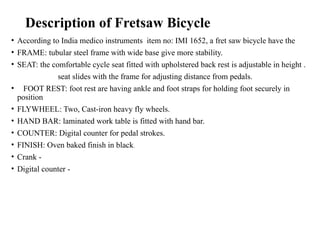
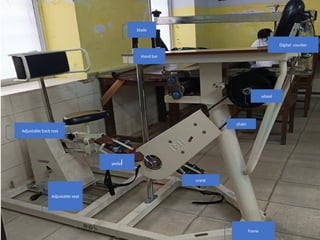
• A bicycle fret saw machine is operated by means of cycle
chain activated by patient through cycling motion. Smooth
pedaling action aided with heavy fly wheel provides low
inertia for early treatment. [Integrated Bio-Medics &
Technologies (IBMT)]
• Fret-saw.
1. A saw with a relatively long, narrow blade, used in cutting
the thin woods, etc.](https://image.slidesharecdn.com/bicyclefretsaw-241028194056-c4ef3a03/85/Bicycle_Fretsaw_-pptx-Static-cycle-for-endurance-training-2-320.jpg)
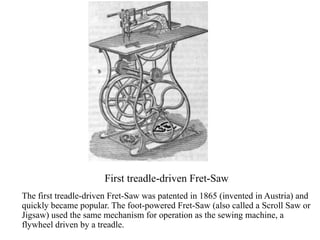
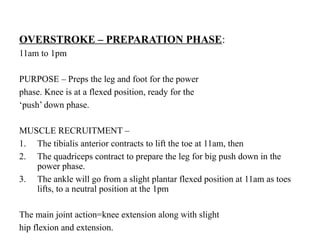
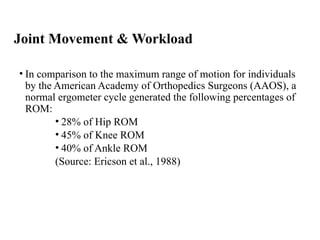
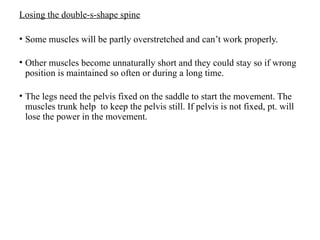
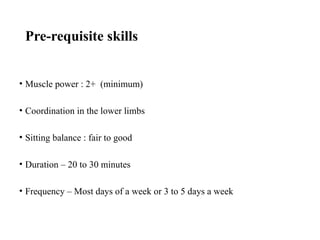
![Muscle Activity During Cycling
[Acc. to Ryan & Gregor (1992)]
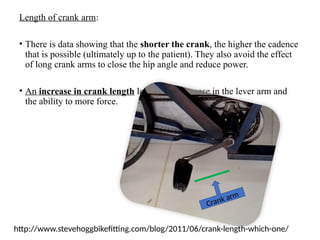
Fig: Overview of muscle activity timing in lower extremities during cycling in relation
to the crank angle (1=TA, 2=SOL, 3=GM, 4=VL&VM, 5=RF, 6=BF and 7=GMax).
Based on the results of Ryan & Gregor, (1992)](https://image.slidesharecdn.com/bicyclefretsaw-241028194056-c4ef3a03/85/Bicycle_Fretsaw_-pptx-Static-cycle-for-endurance-training-18-320.jpg)
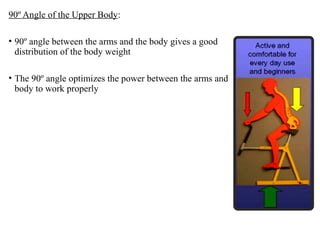
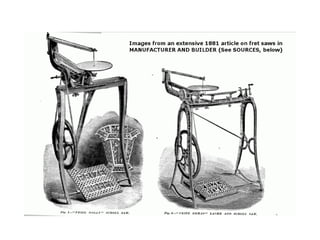
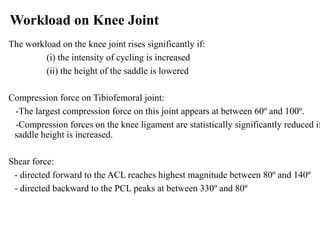
![Muscle Activity During Cycling
[Acc. to Ryan & Gregor (1992)]
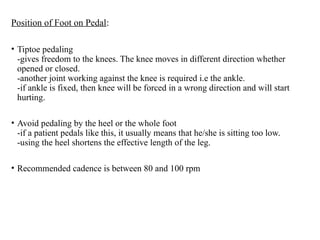
• (1=TA, 2=SOL, 3=GM, 4=VL&VM, 5=RF,
6=BF and 7=GMax).
• GMax extends the hip
-active between 340º and 130º
-peaking at 80º
• VL & VM extends the knee
-active between 300º and 130º
-peaking at 30º
• RF acts as knee extensor & hip flexor
-active between 200º and 110º
-peaking at 20º](https://image.slidesharecdn.com/bicyclefretsaw-241028194056-c4ef3a03/85/Bicycle_Fretsaw_-pptx-Static-cycle-for-endurance-training-19-320.jpg)
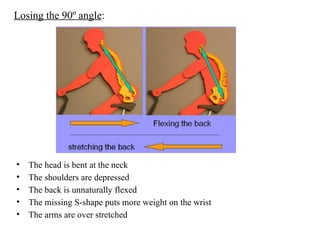
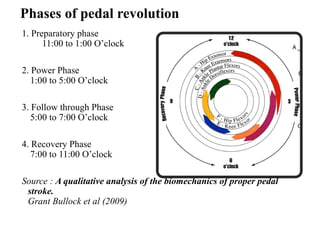
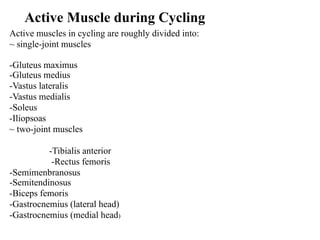
![Muscle Activity During Cycling
[Acc. to Ryan & Gregor (1992)]
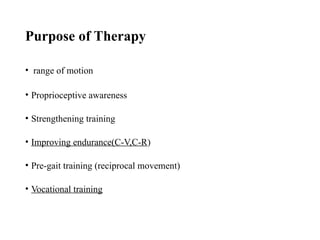
• SOL stabilizes the ankle joint
-active between 340º and 270º
-peaking at 90º when the forces exerted on
the pedal are the highest.
• GM & GL both flexes the knee and
stabilization of ankle joint
-active between 350º and 270º
-peaking at 110º
• TA stabilizes and flexes the ankle joint
-active throughout cycle
-peaking at 280º](https://image.slidesharecdn.com/bicyclefretsaw-241028194056-c4ef3a03/85/Bicycle_Fretsaw_-pptx-Static-cycle-for-endurance-training-20-320.jpg)
![Muscle Activity During Cycling
[Acc. to Ryan & Gregor (1992)]
• SM & ST flexes the knee
-active between 10º and 230º
-peaking at 100º
• BF flexes the knee and extends the
hip
-active between 350º and 230º
-peaking at 110º](https://image.slidesharecdn.com/bicyclefretsaw-241028194056-c4ef3a03/85/Bicycle_Fretsaw_-pptx-Static-cycle-for-endurance-training-21-320.jpg)