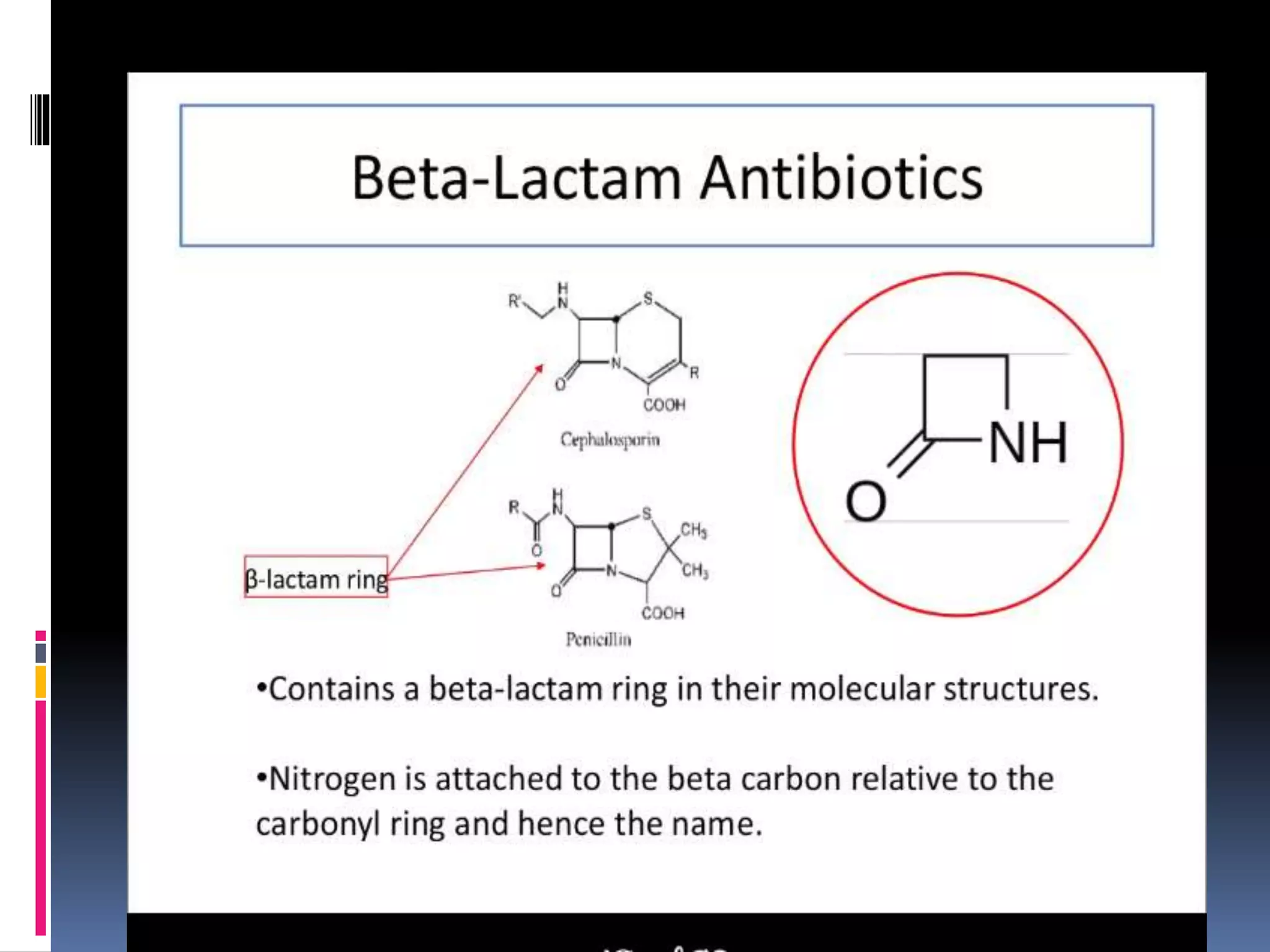
This document provides an overview of beta lactam antibiotics, including penicillins, semisynthetic penicillins, cephalosporins, monobactams, and carbapenems. It describes their classification, mechanisms of action, therapeutic uses, doses, and side effects. Beta lactam antibiotics work by inhibiting cell wall synthesis in bacteria. Penicillins are the oldest and include natural penicillins along with semisynthetic derivatives like methicillin and amoxicillin. Cephalosporins have a similar structure and mode of action as penicillins. Newer classes include monobactams and carbapenems, which are effective against hospital-acquired infections.
















































![RIFAMPICIN [MEDICINAL CHEMISTRY] BY P.RAVISANKAR.](https://cdn.slidesharecdn.com/ss_thumbnails/rifampicinppt-ravi-copy-130615225737-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)















































