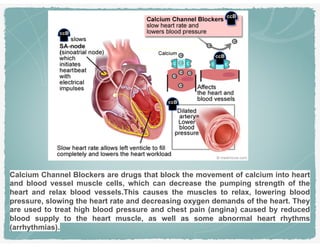
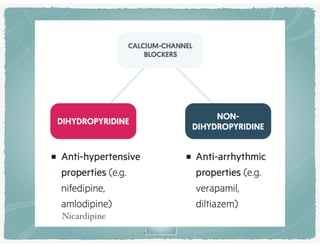
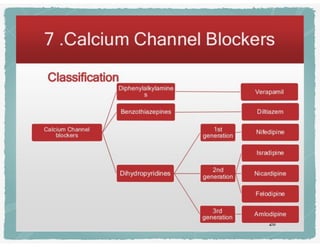
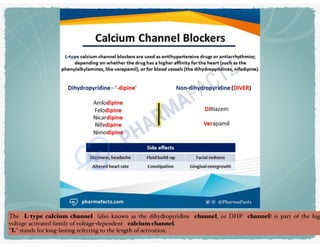
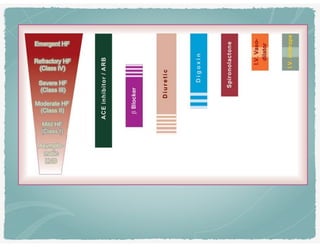
The document provides an overview of cardiovascular drugs, focusing on beta-blockers and calcium channel blockers, discussing their mechanisms, effects on heart rate, and indications for use. It highlights specific medications like nicardipine, verapamil, and diltiazem, detailing their actions, benefits in treating hypertension and angina, and potential side effects. Additionally, it mentions the management of diabetes-related issues and the role of potassium channel openers in hypertension treatment.




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













