Downloaded 22 times


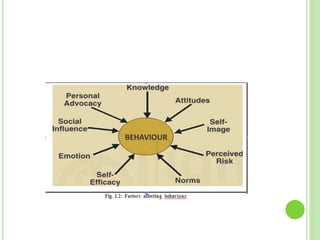


The document outlines the process of communication in health education, emphasizing the importance of effective messaging for behavior change to improve health outcomes. It discusses factors influencing health behavior, the Health Belief Model, and the Transtheoretical Model of Change, as well as strategies and principles for planning behavior change communications. Furthermore, it highlights the need for stakeholder involvement, formative assessments, and continuous evaluation to ensure that communication efforts meet the needs of target populations effectively.












































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









