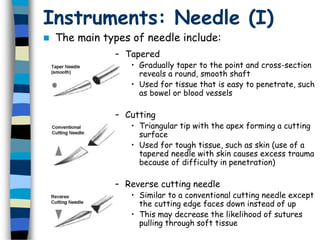
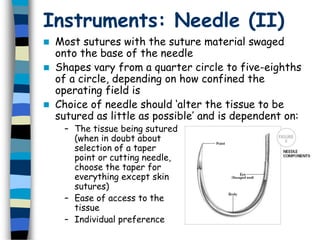
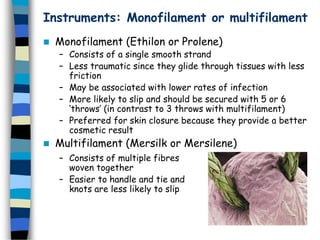
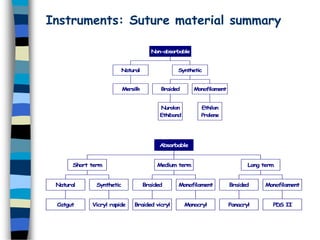
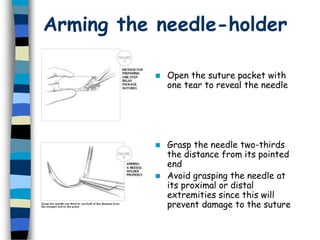
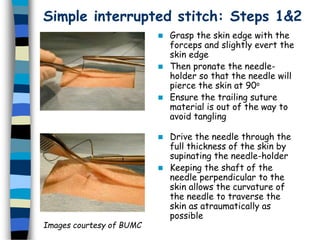
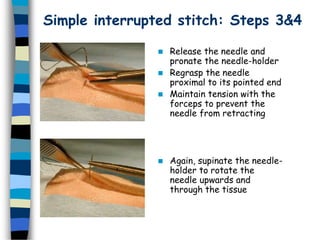
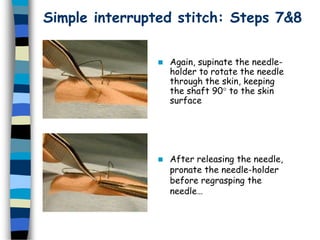
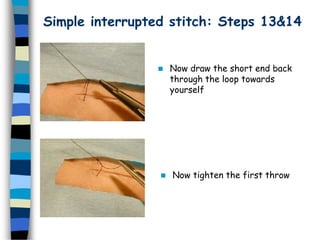
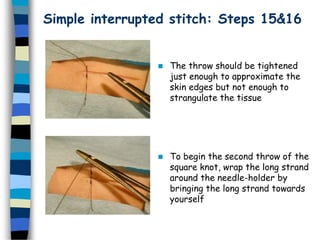
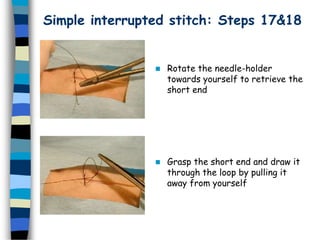
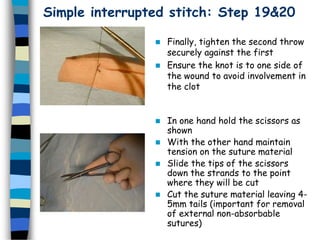
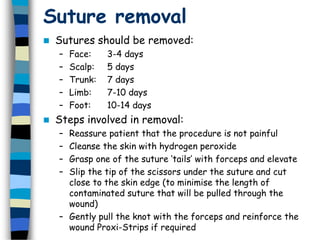
This document provides an overview of basic surgical skills related to wound classification, types of wound healing, suturing instruments and materials, and suturing technique. It describes the CDC classification system for wounds as clean, clean-contaminated, contaminated, or infected. The types of wound healing are defined as primary intention, secondary intention, or delayed primary closure. Suturing instruments and materials covered include needle types, suture properties, sizes and compositions. The simple interrupted suturing technique is demonstrated in 20 steps. Guidelines for suture removal are also provided.