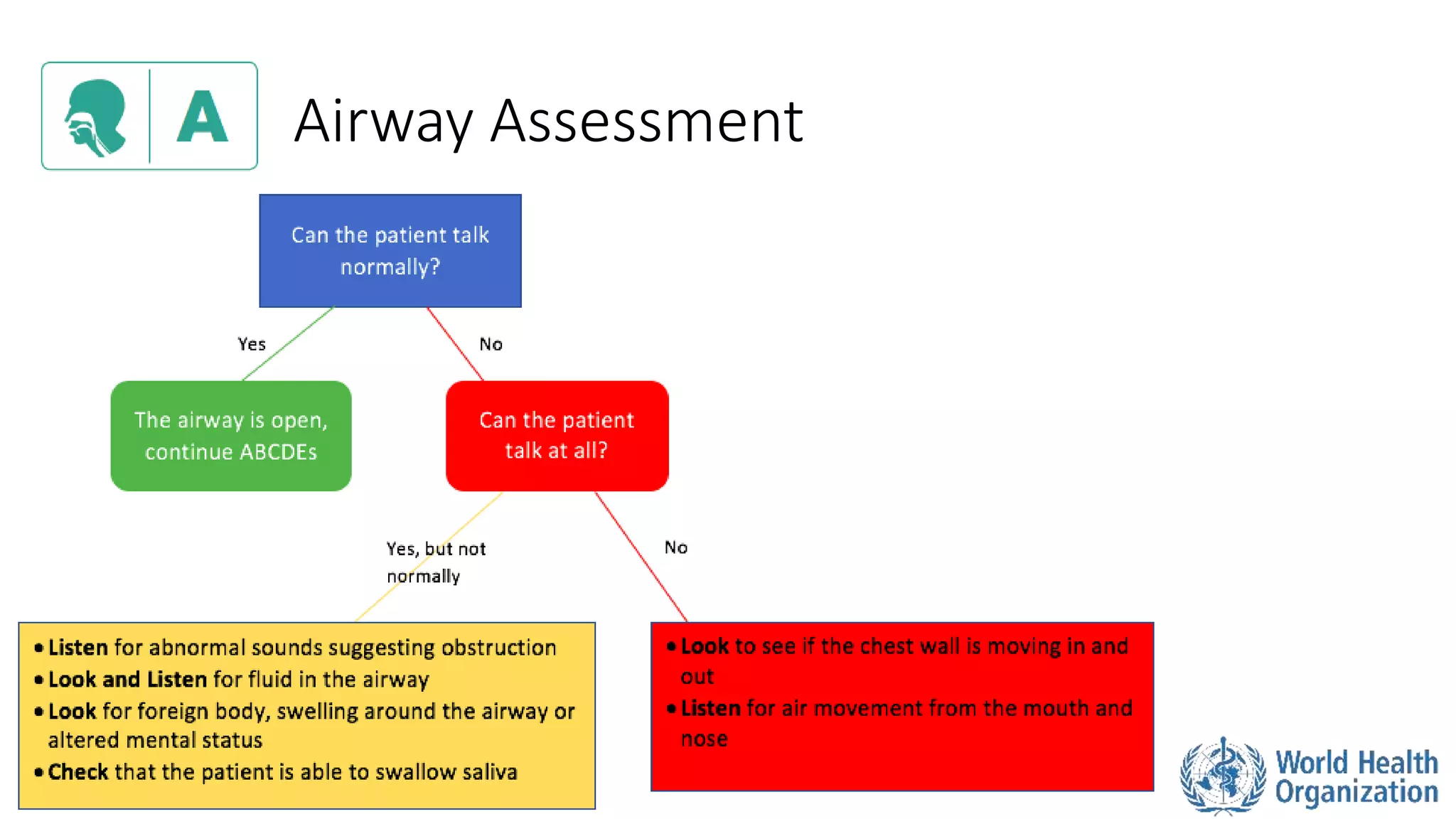
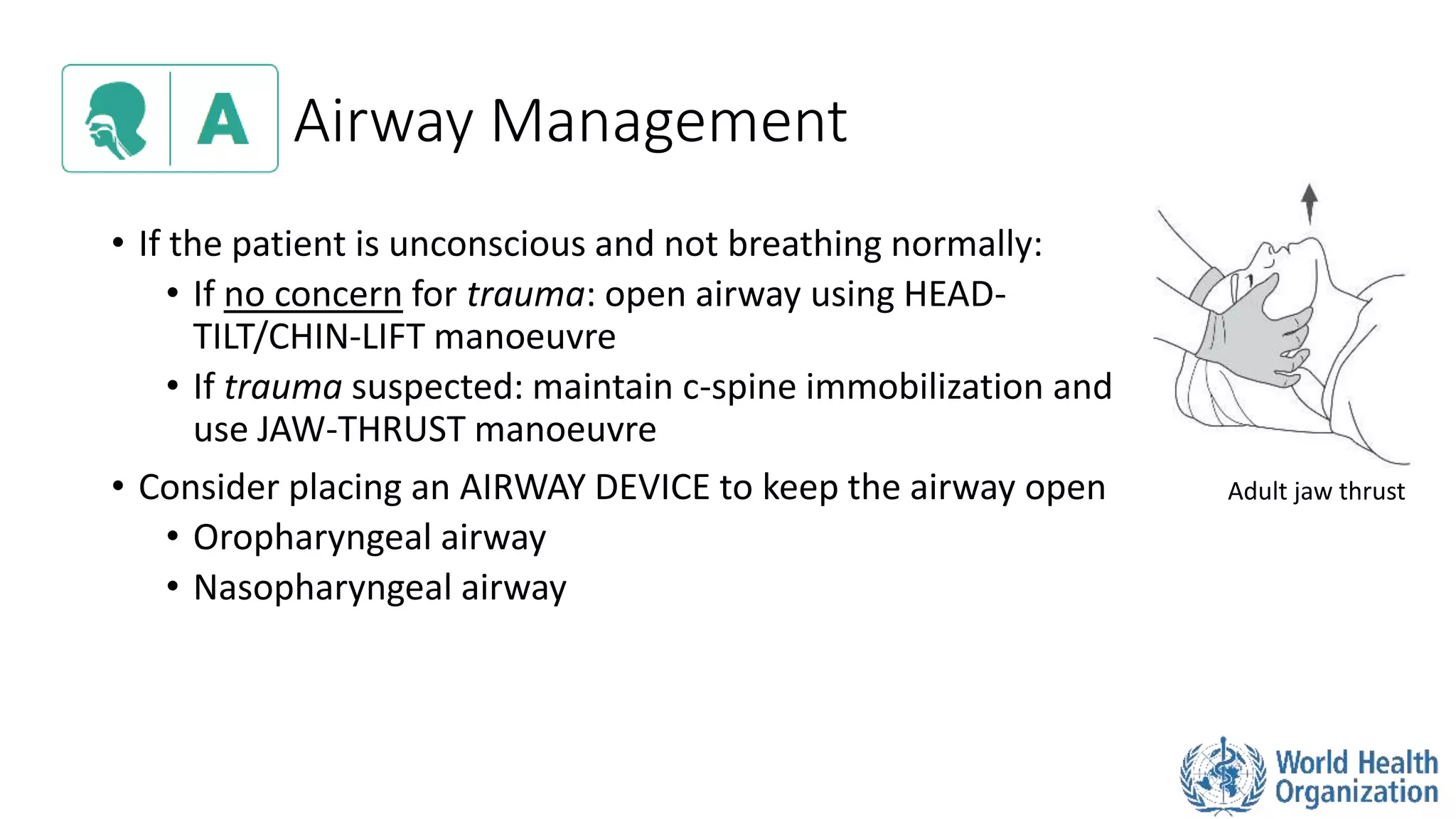
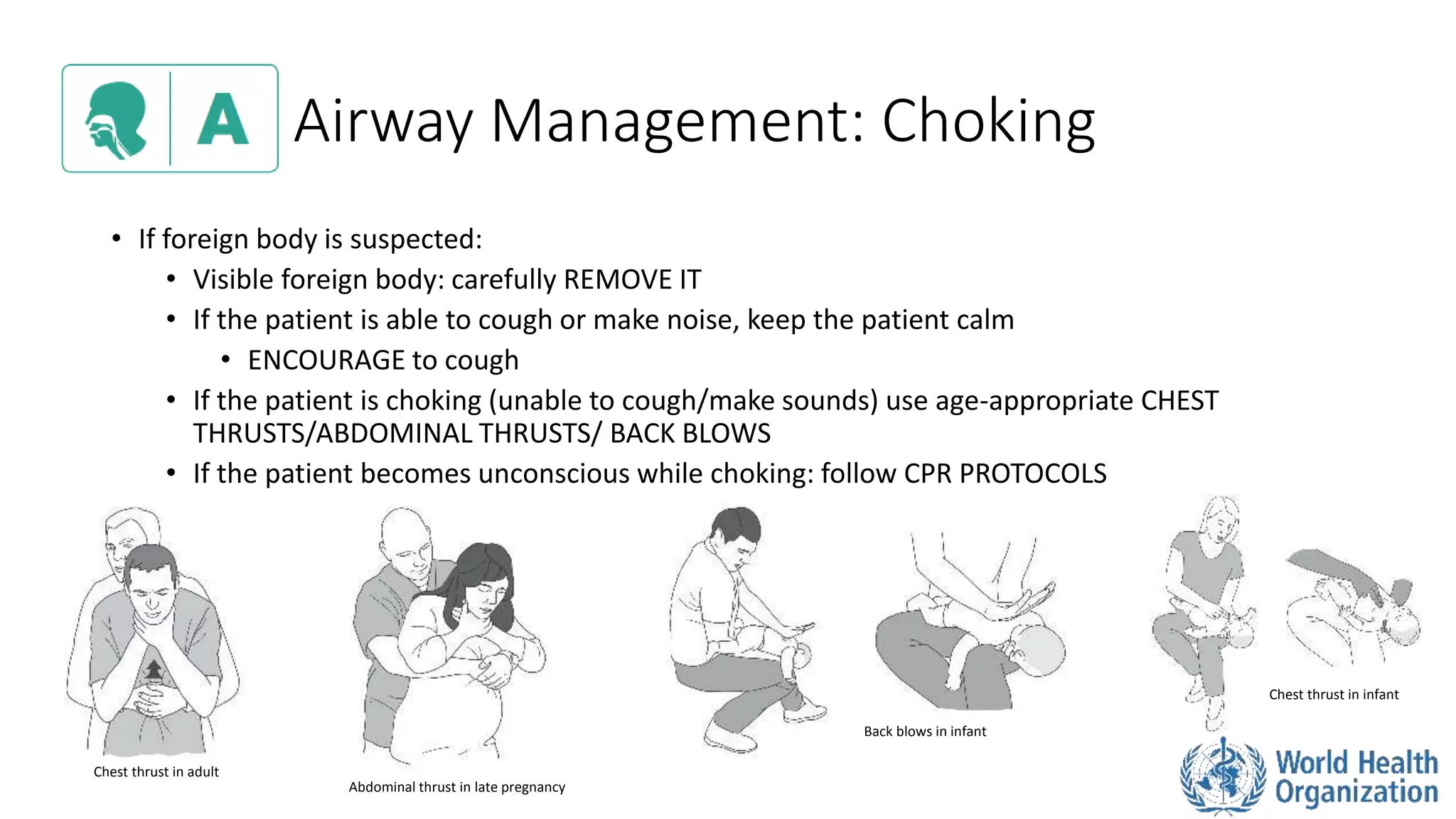
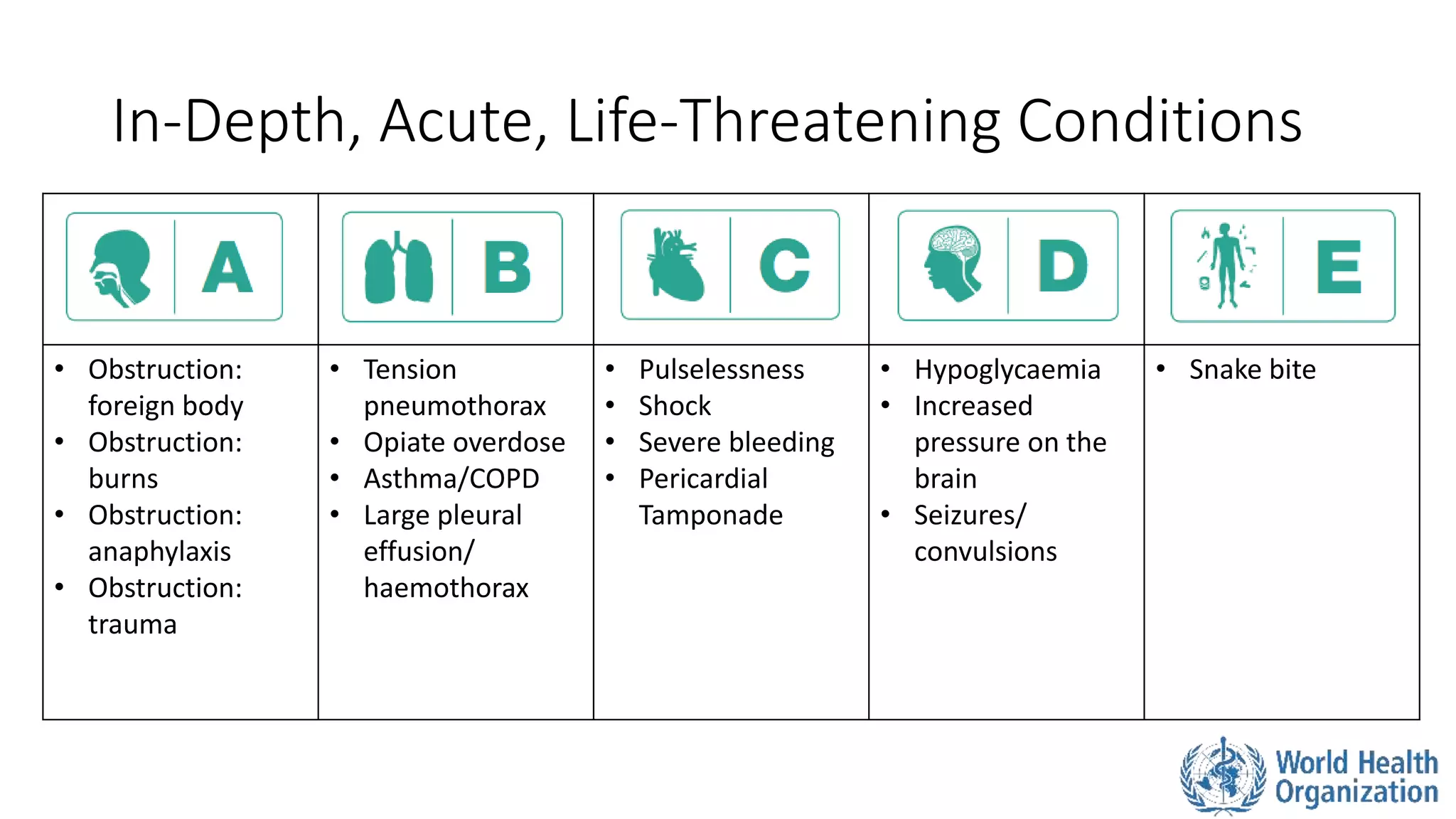
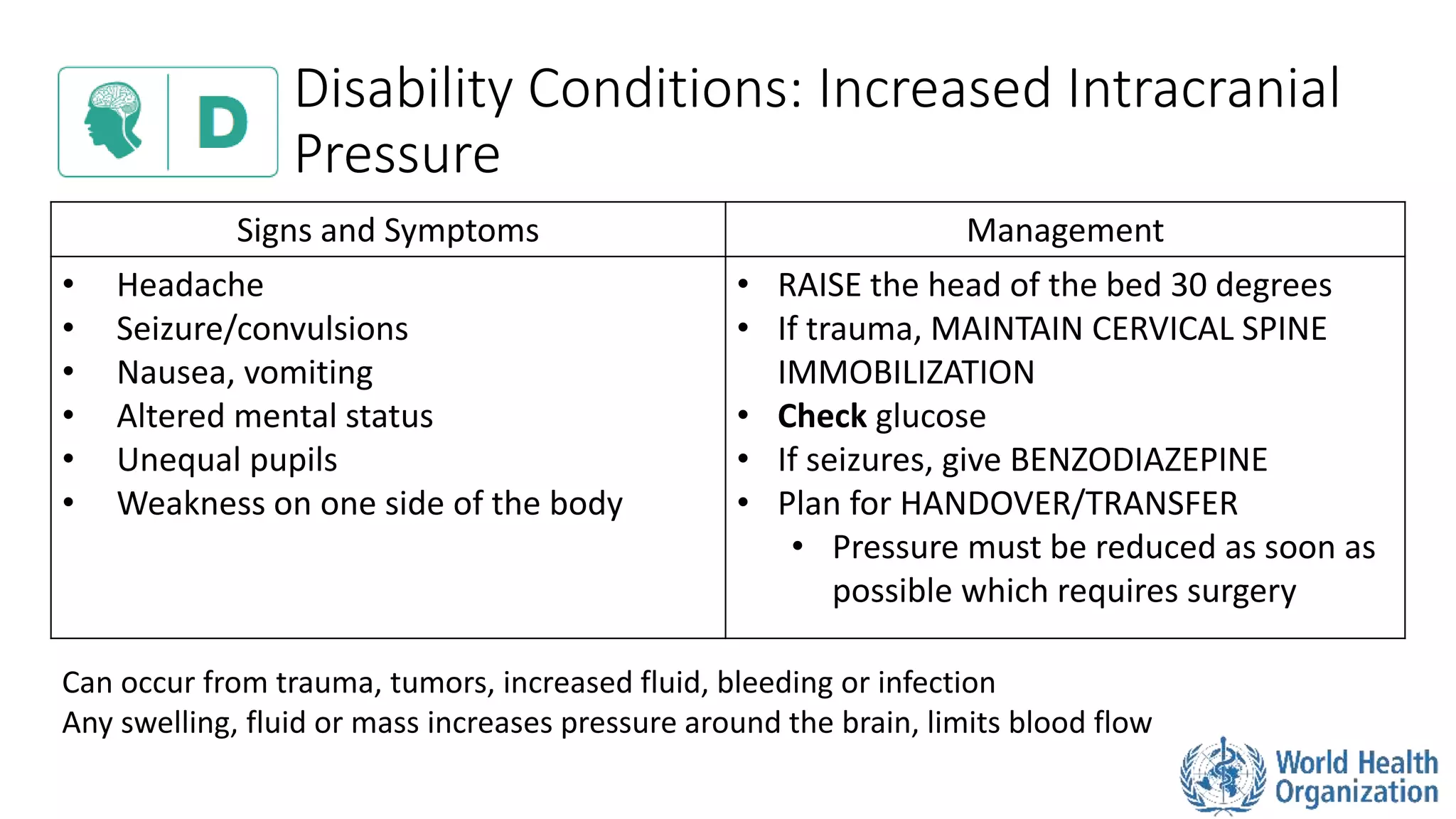
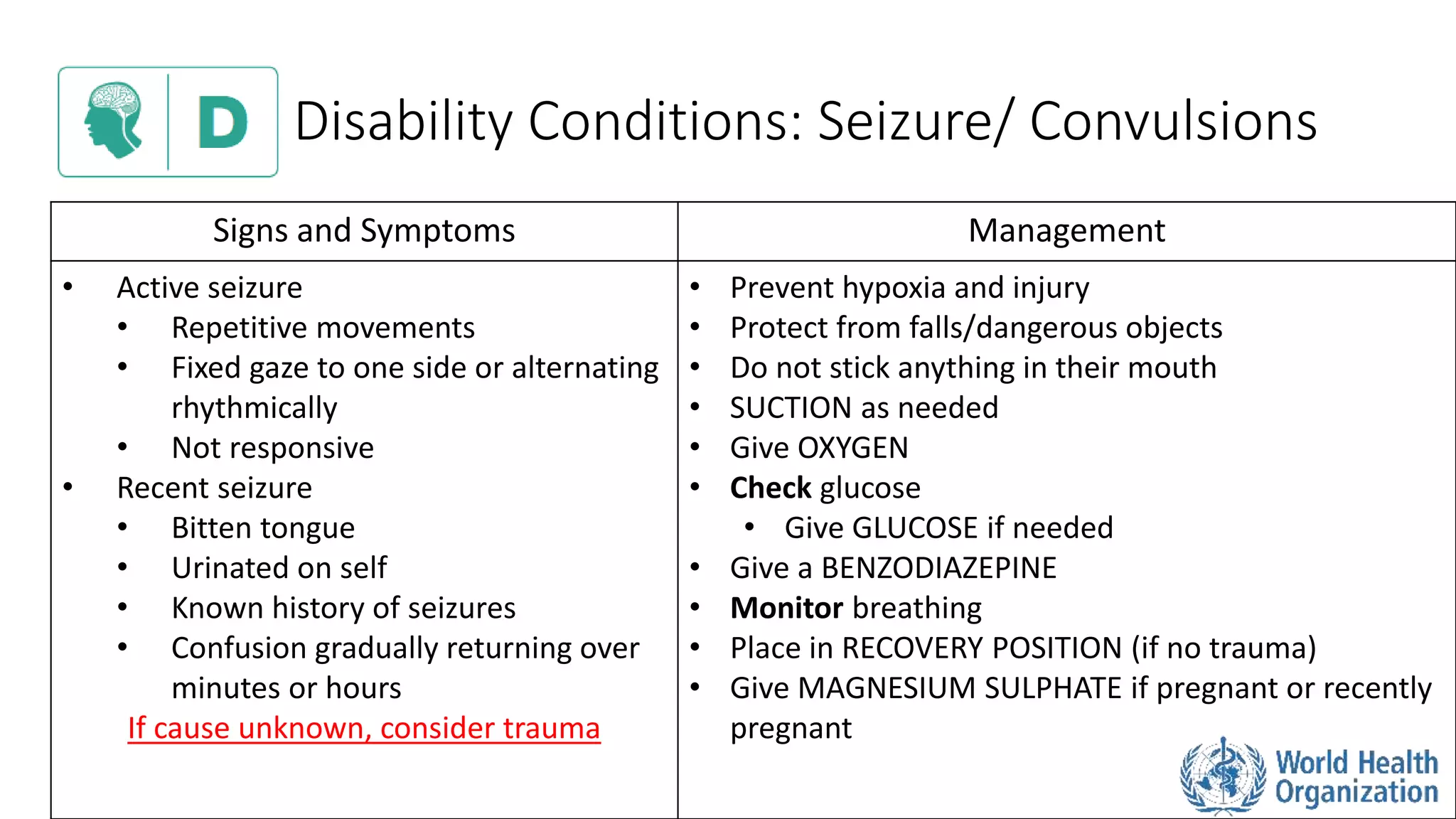
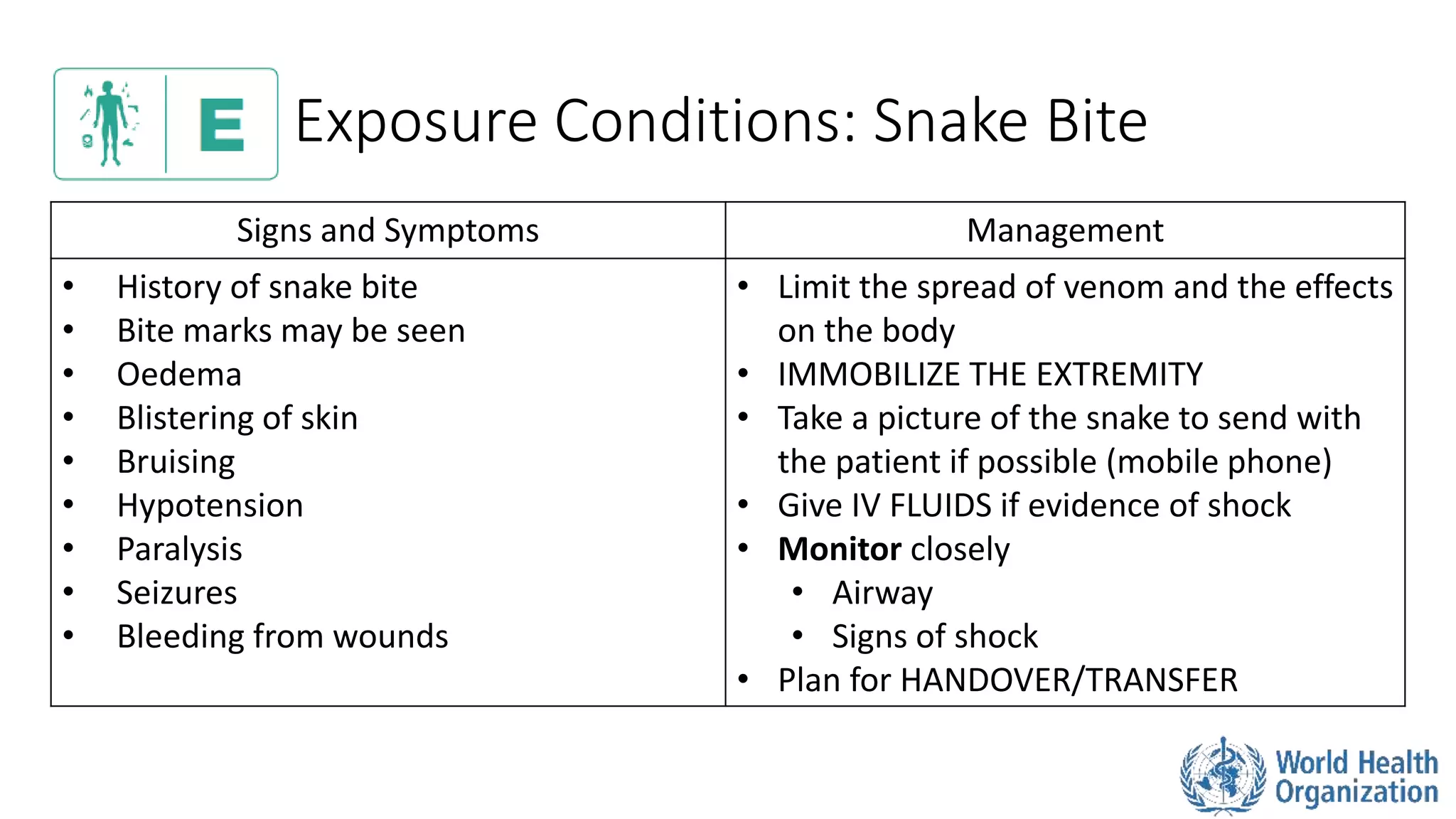
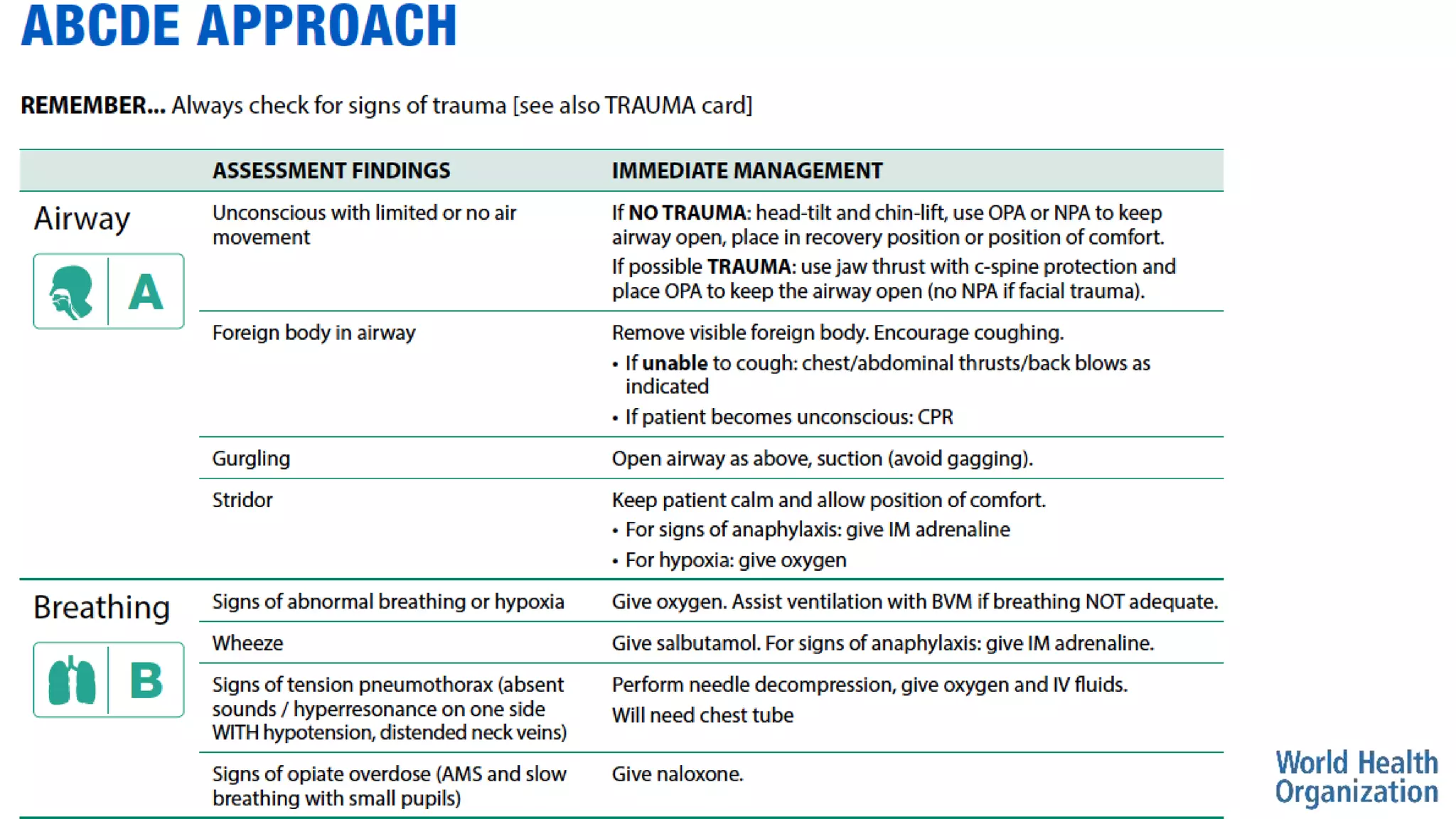
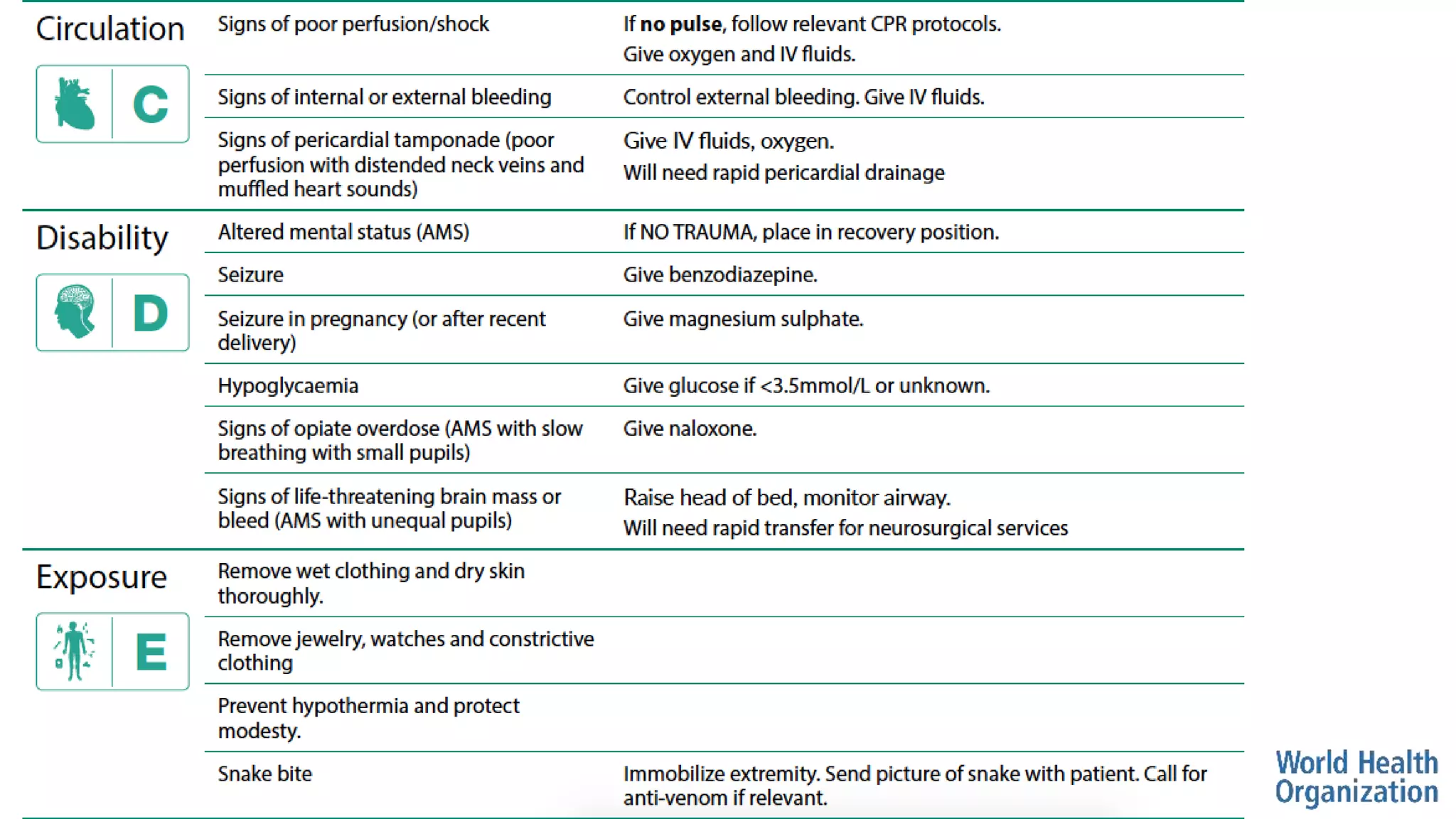
The document outlines the ABCDE and SAMPLE history approach for assessing and managing emergency patients, with the ABCDE approach assessing the airway, breathing, circulation, disability, and exposure, while the SAMPLE history collects information on signs/symptoms, allergies, medications, past medical history, last oral intake, events, and examines the patient. It provides detailed guidance on evaluating and treating life-threatening conditions in each area, such as managing an obstructed airway, breathing difficulties, shock, or altered mental status. The goal is to rapidly identify and address critical issues through this systematic approach.



































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)
















