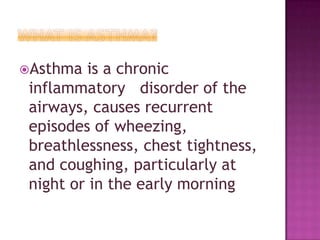
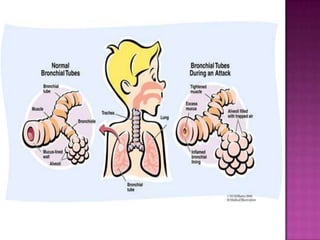
This document discusses asthma and its implications for dental treatment. It defines asthma as a chronic inflammatory airway disease characterized by wheezing, breathlessness, and coughing. It notes several triggers that can cause an asthmatic attack during dental procedures and recommends ways to prevent and treat such attacks, such as using asthma medications prophylactically, avoiding triggers, and having emergency medications on hand. The document emphasizes the importance of communication with asthmatic patients and recognizing signs of an attack to provide prompt treatment.




































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


