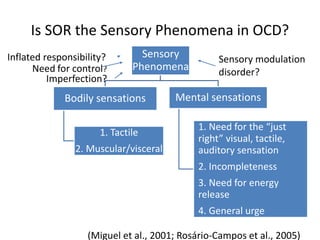
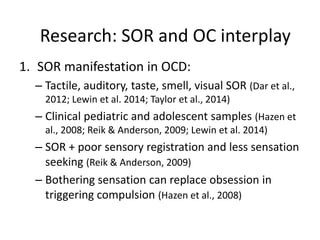
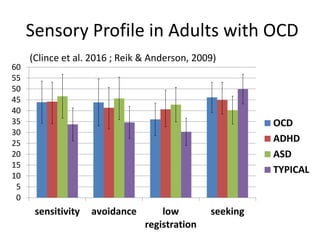
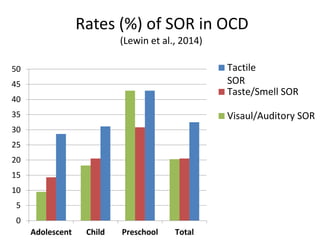
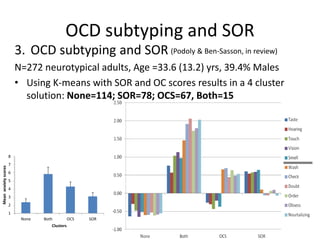
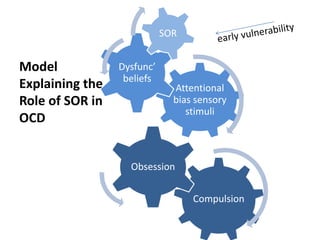
1) Sensory over-responsivity (SOR) is a type of sensory processing disorder involving negative responses to daily sensations. Research shows SOR is prevalent in OCD and associated with greater OCD severity and specific compulsion types.
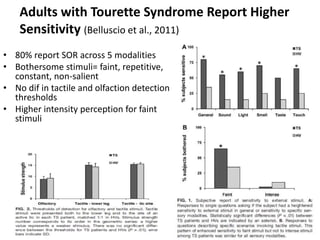
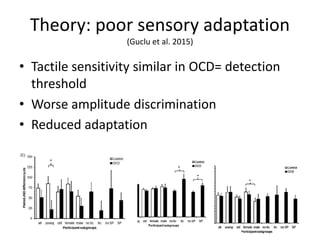
2) Theories suggest SOR creates attentional biases towards stimuli leading to obsessive thoughts and compulsions. Poor sensory adaptation may also underlie the SOR-OCD relationship.
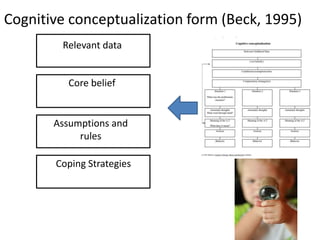
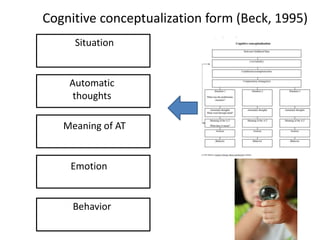
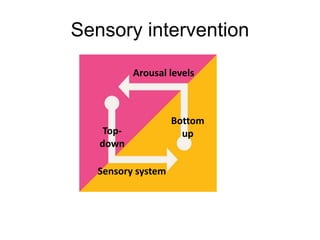
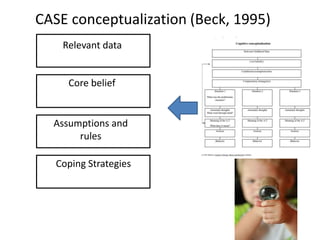
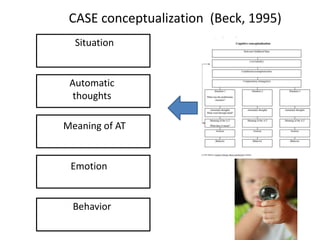
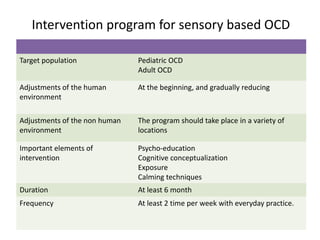
3) Sensory-based assessment and treatment involves identifying SOR, cognitive conceptualization, graded exposure, and calming techniques to prevent avoidance and regulate arousal. Treatment is multi-phasic and targets regulation of sensations, thoughts, and behaviors.










![Etiopathogenesis of obsessive compulsive disorder [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/etiopathogenesisofobsessivecompulsivedisorderautosaved-170329074058-thumbnail.jpg?width=640&height=640&fit=bounds)











































































