Downloaded 82 times
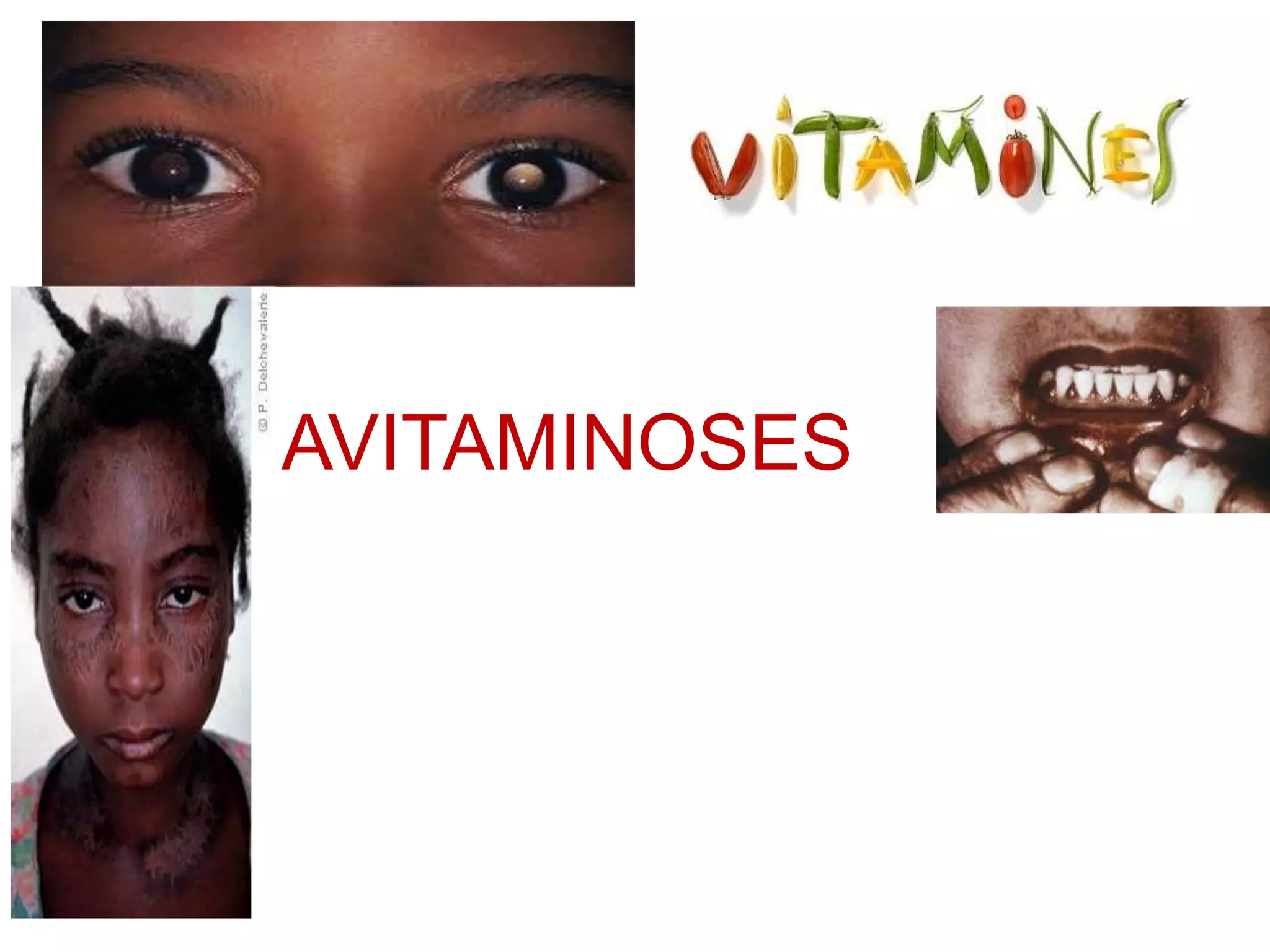




























The document discusses the importance of vitamins, their classifications into fat-soluble and water-soluble categories, and the diseases associated with their deficiencies, known as avitaminoses. It details specific vitamins such as A, D, E, K, C, and B-complex, their roles, deficiency conditions, and oral manifestations. The conclusion emphasizes that most deficiency-related diseases can be reversed through adequate dietary intake.