Download as PDF, PPTX

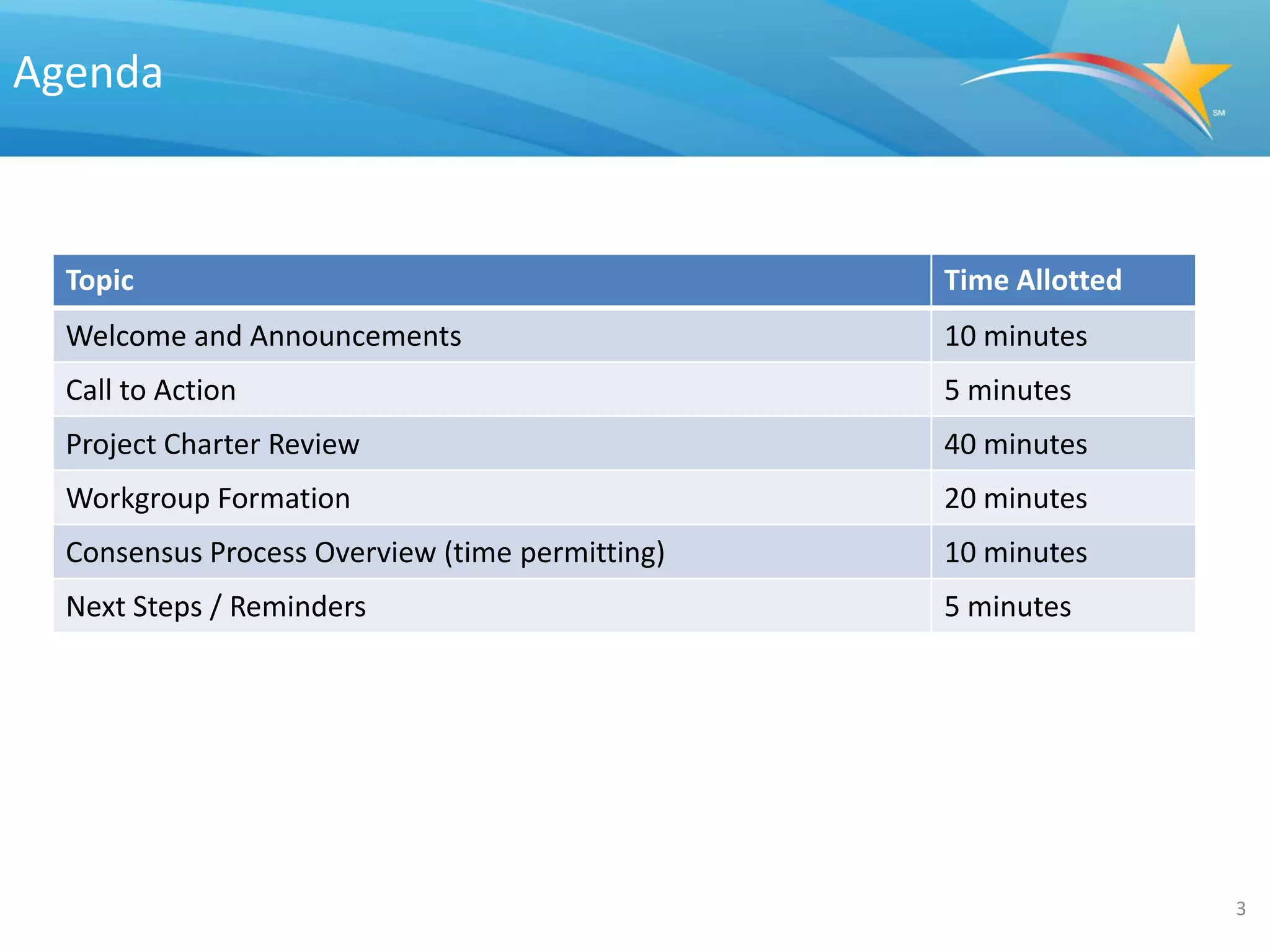


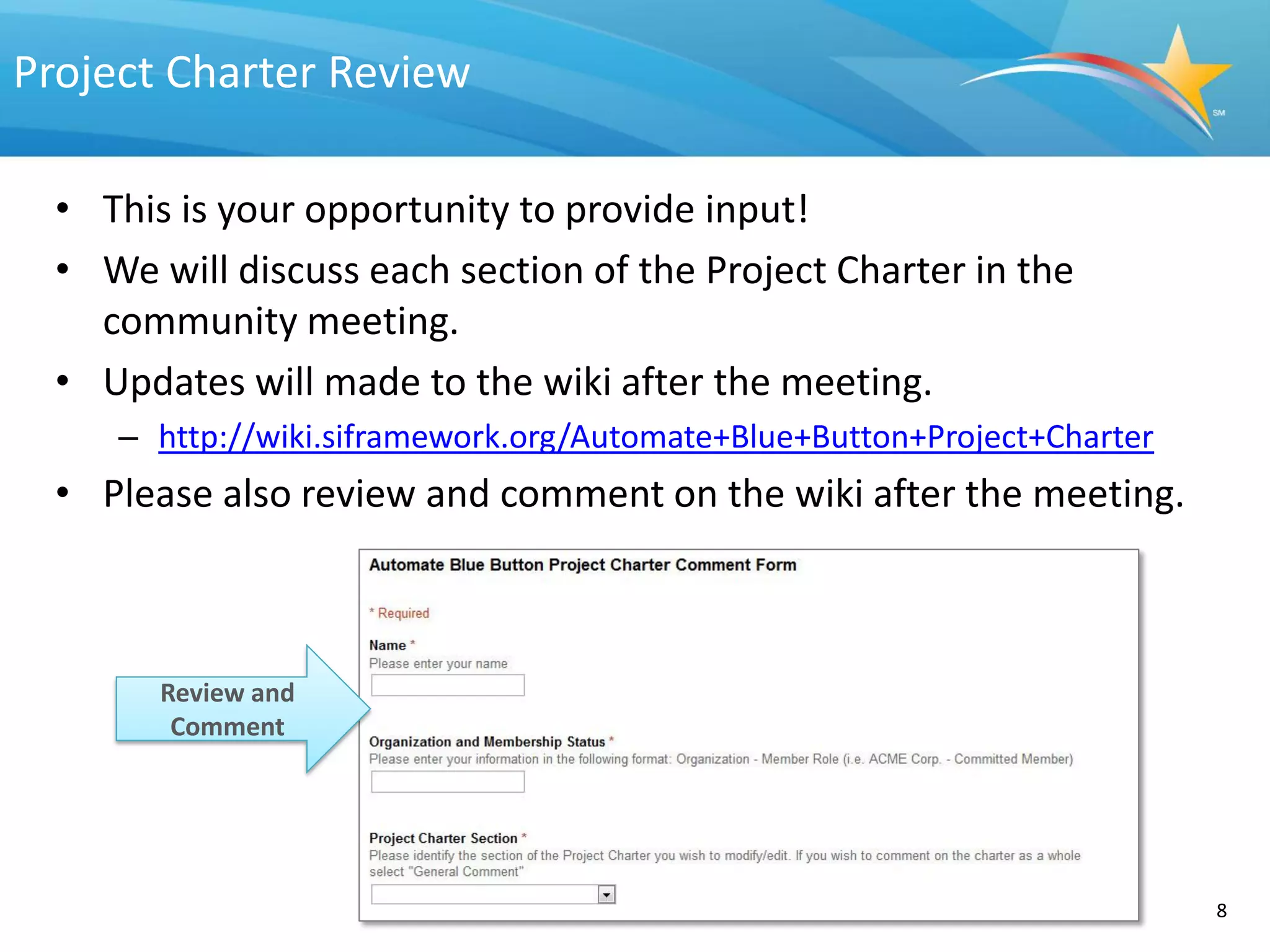
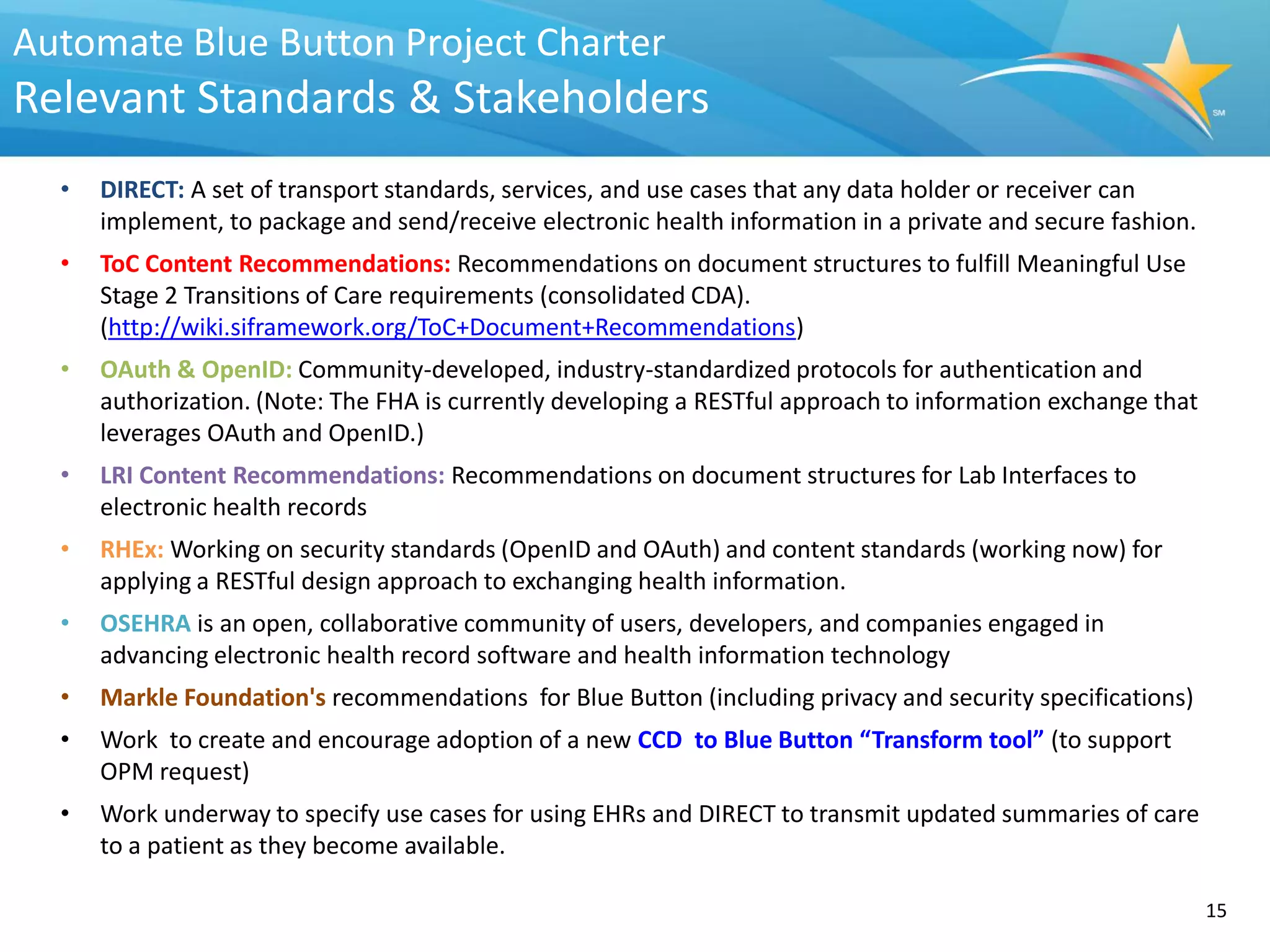
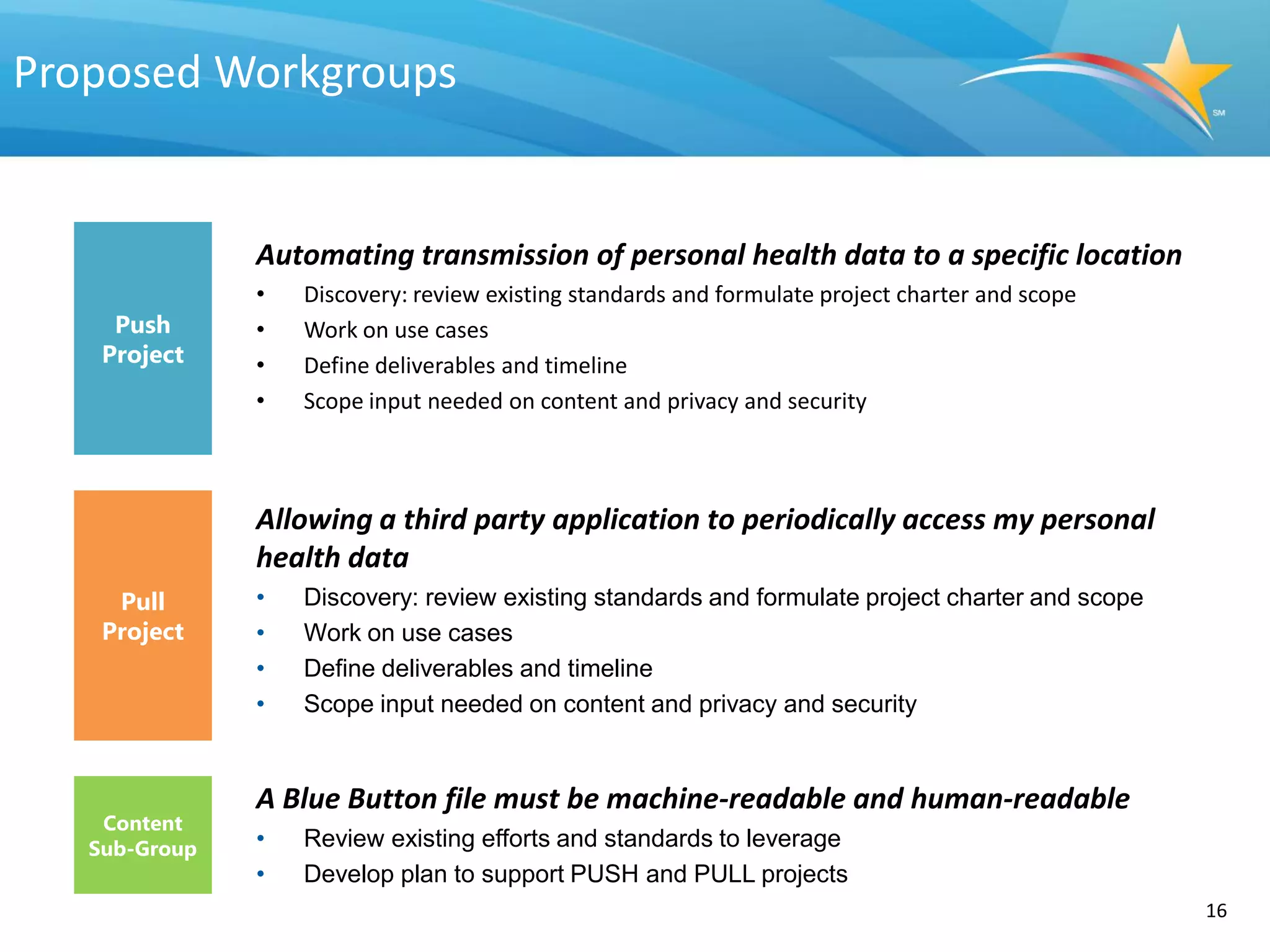
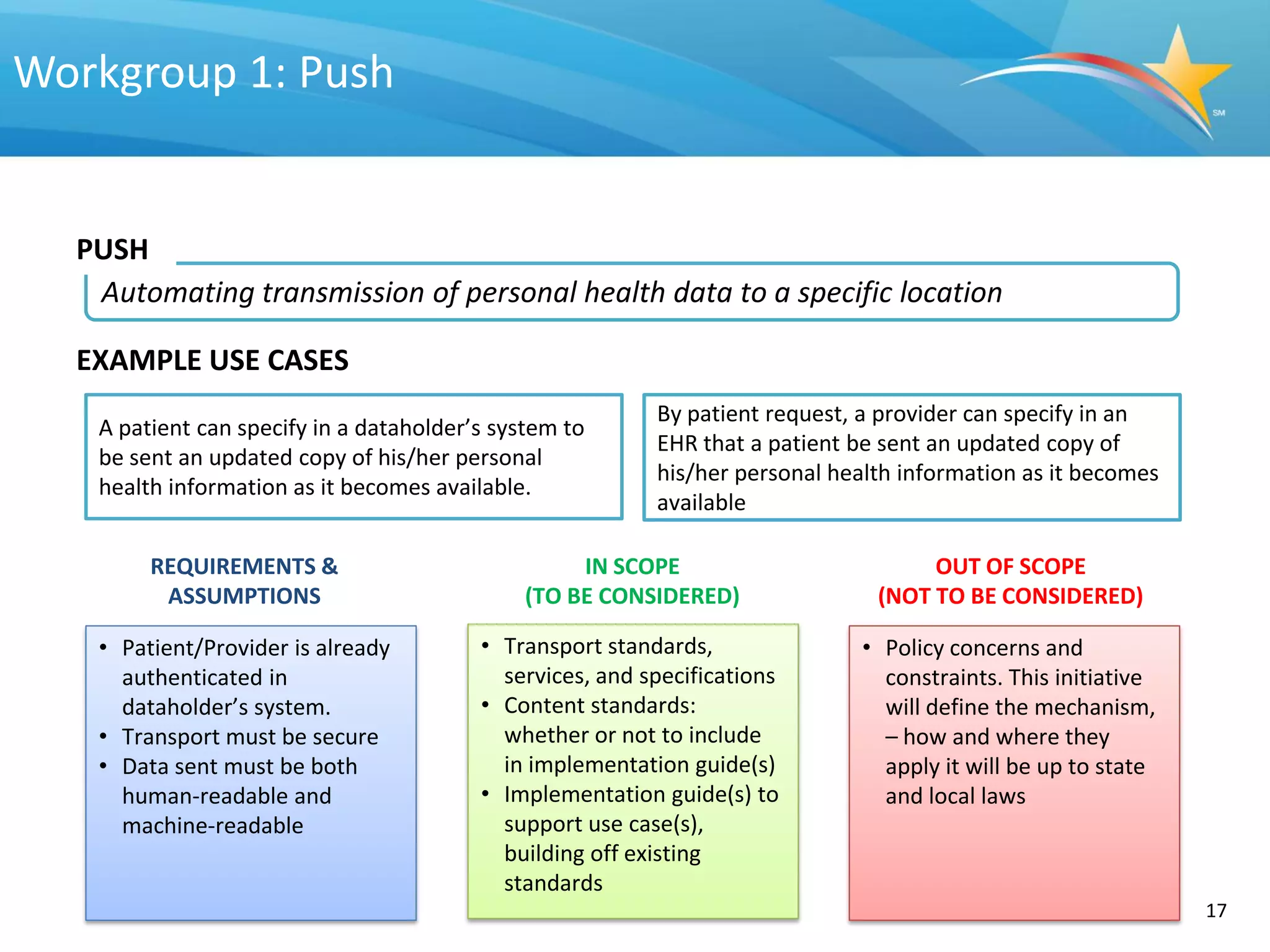
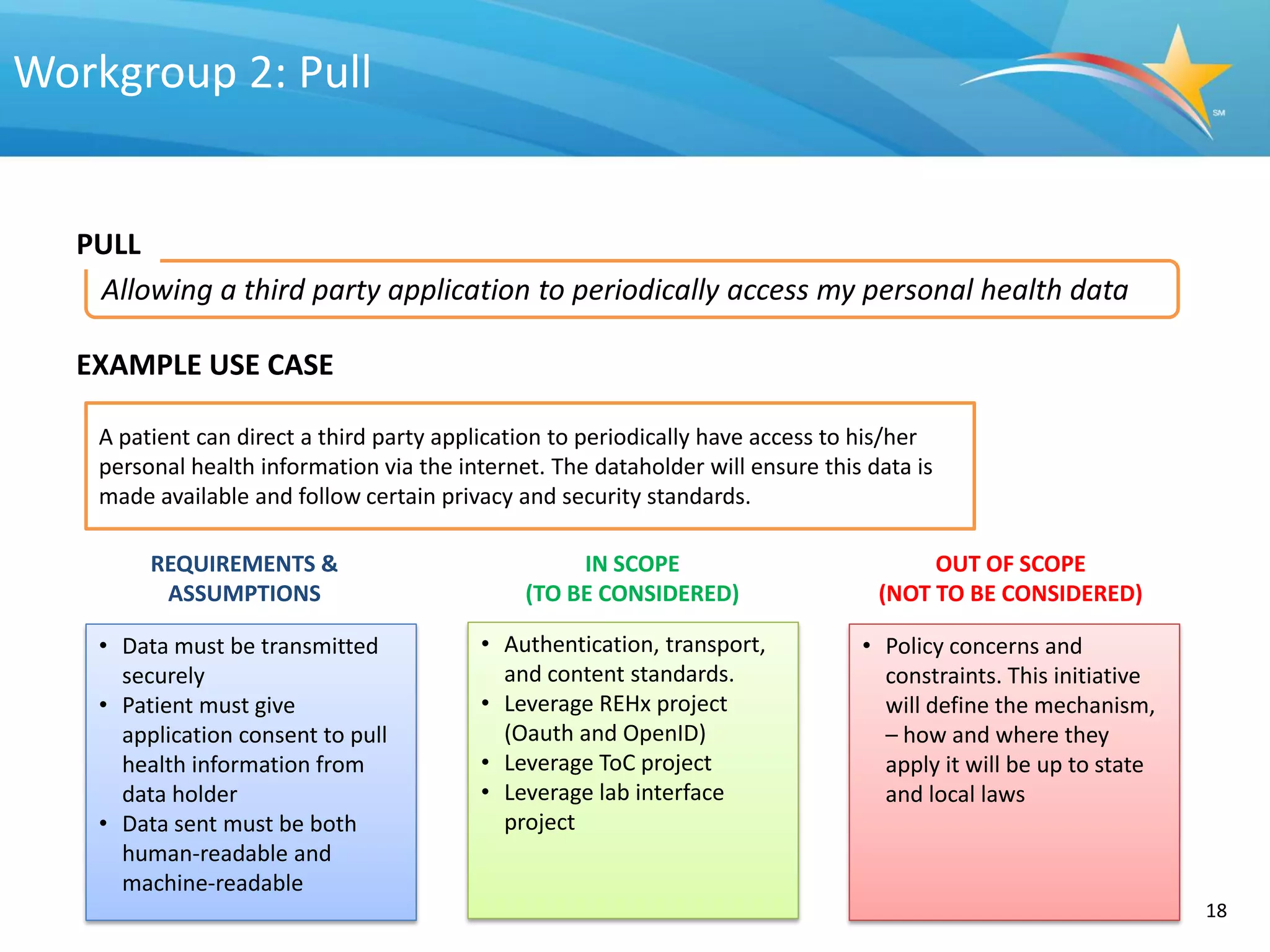
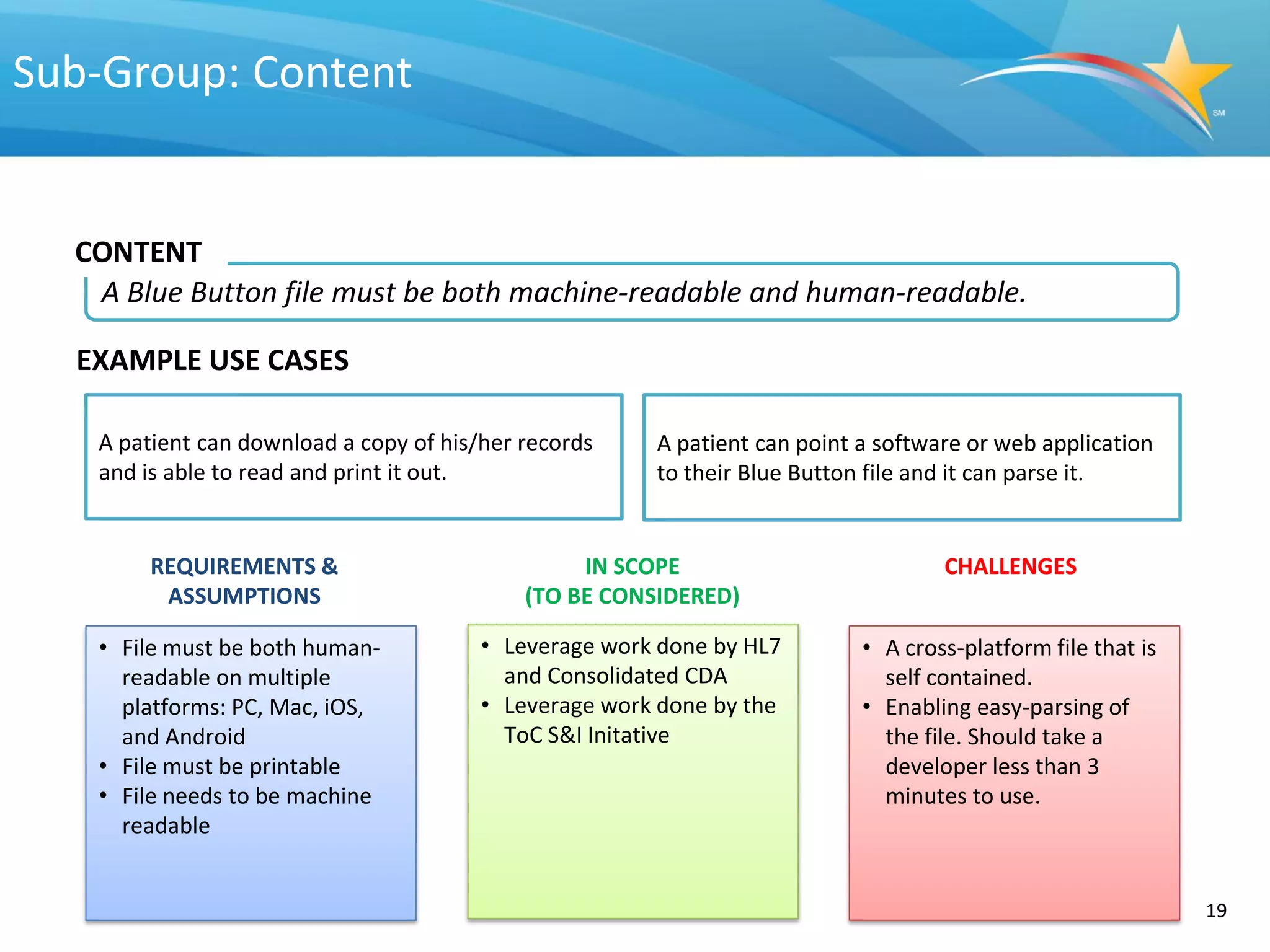
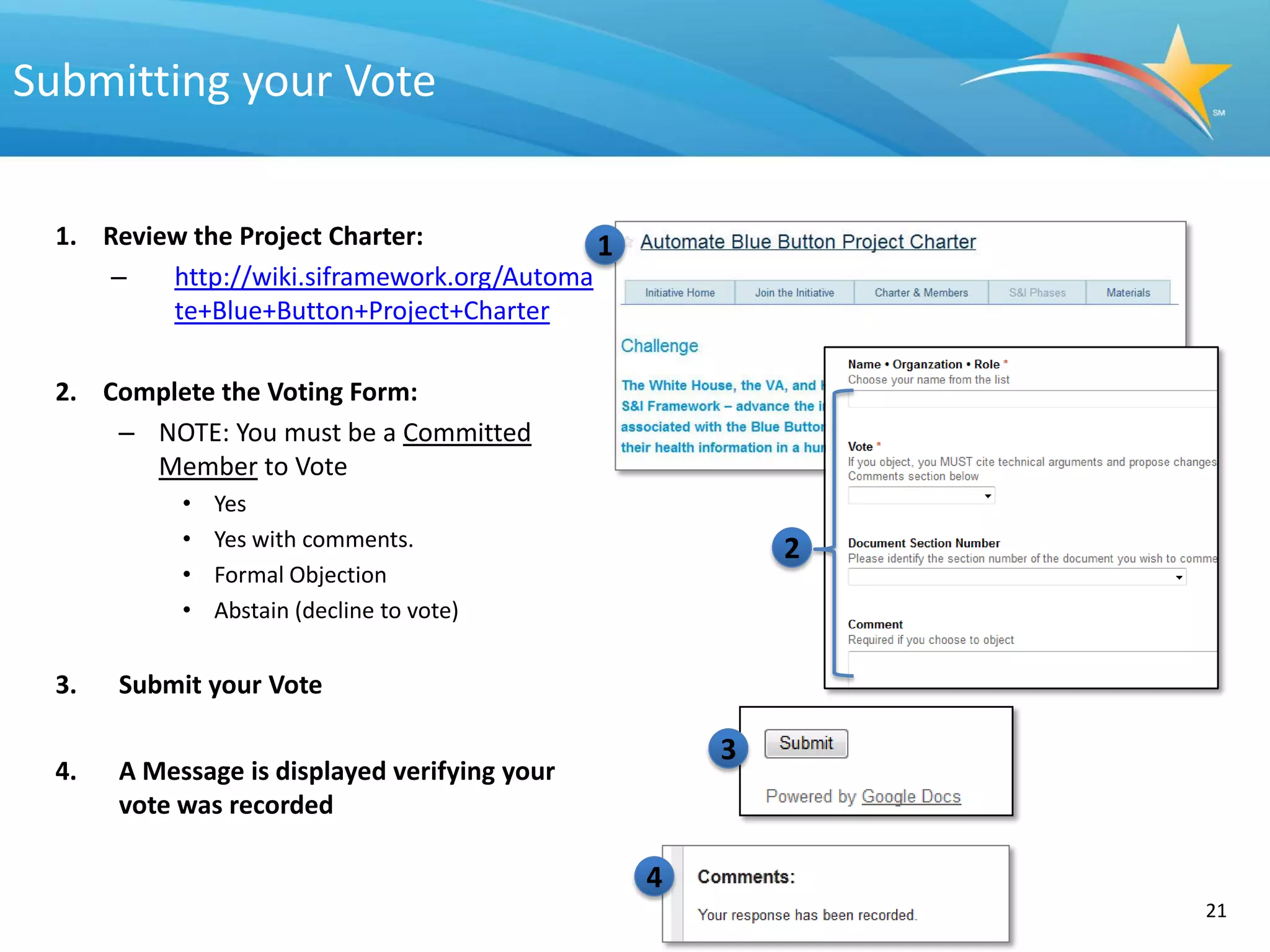
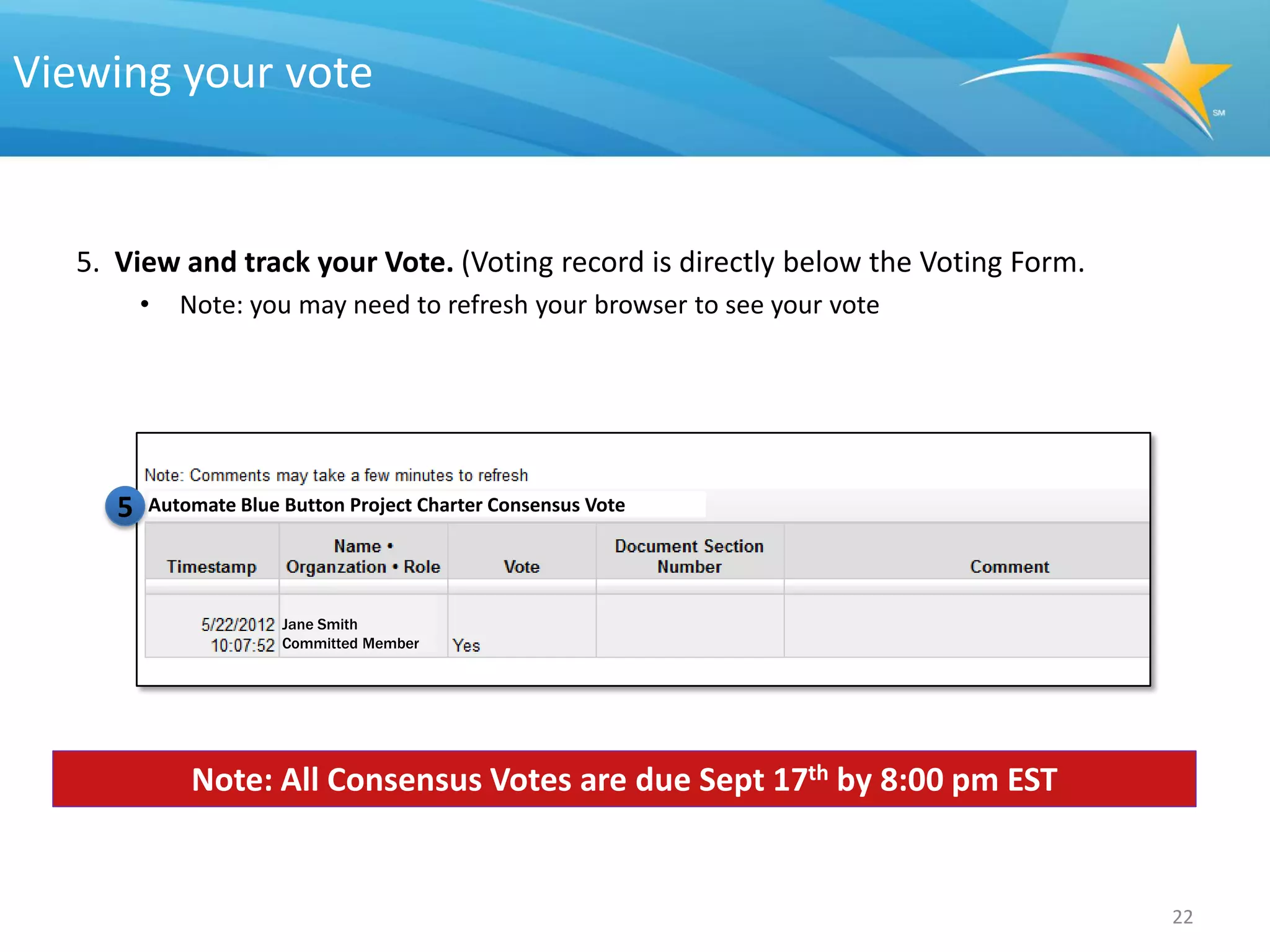

This document provides an overview of an upcoming community meeting to discuss the Automate Blue Button Initiative project charter. The meeting will include a call to action for participants to join the initiative, a review and discussion of each section of the project charter, and an explanation of relevant standards and stakeholders. The project charter establishes the challenge of automating the transmission and access of personal health data via the Blue Button, sets goals and a scope statement, and outlines a value statement, success metrics, milestones, deliverables, and standards. Participants are invited to review and provide input on the charter sections.



























































































