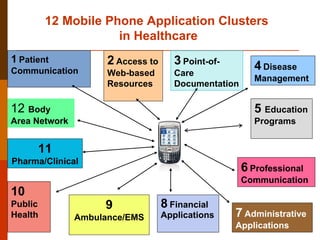
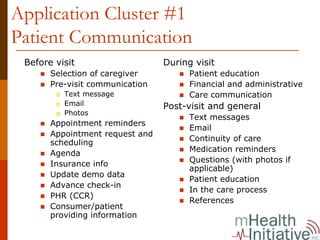
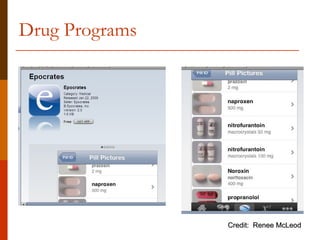
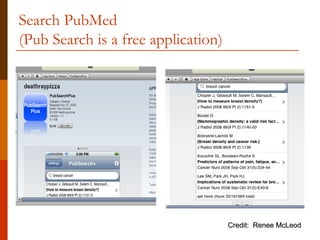
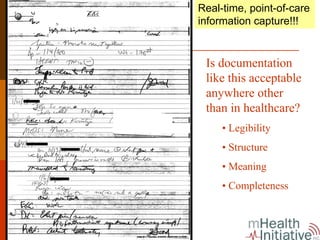
The document summarizes 12 clusters of mobile health (mHealth) applications for healthcare. It describes each cluster including patient communication applications, access to web-based resources, point-of-care documentation, disease management, education programs, professional communication, administrative applications, financial applications, emergency care, public health applications, pharmaceutical/clinical trials applications, and body-area networks. For each cluster, it provides examples of current applications and considerations for developing standards and evaluating the applications. The document was presented at an mHealth seminar by the CEO of the mHealth Initiative.


































![Wiredandwireless2 12656614569424 Phpapp02[1]](https://cdn.slidesharecdn.com/ss_thumbnails/wiredandwireless2-12656614569424-phpapp021-100821181644-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)























































