Downloaded 22 times





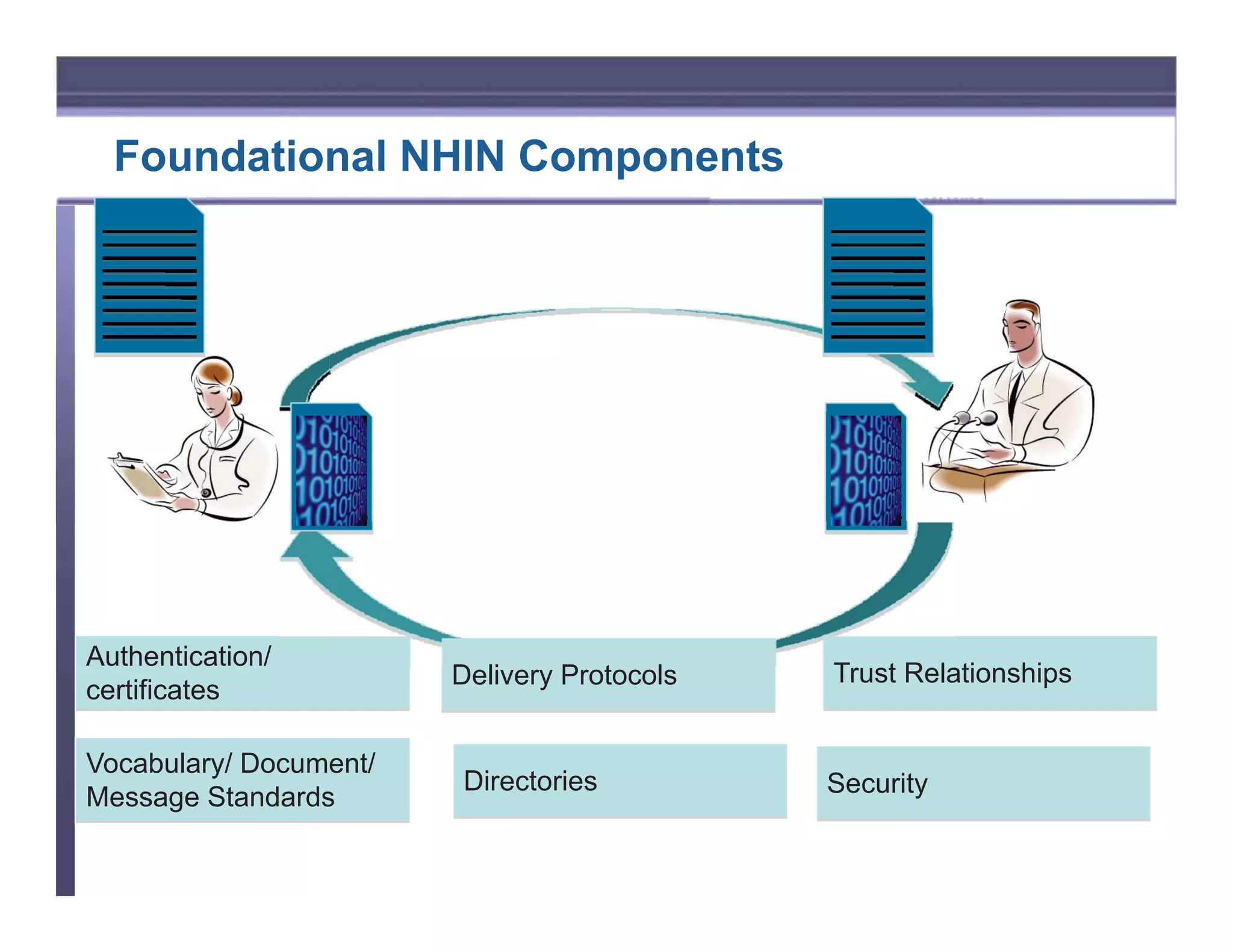









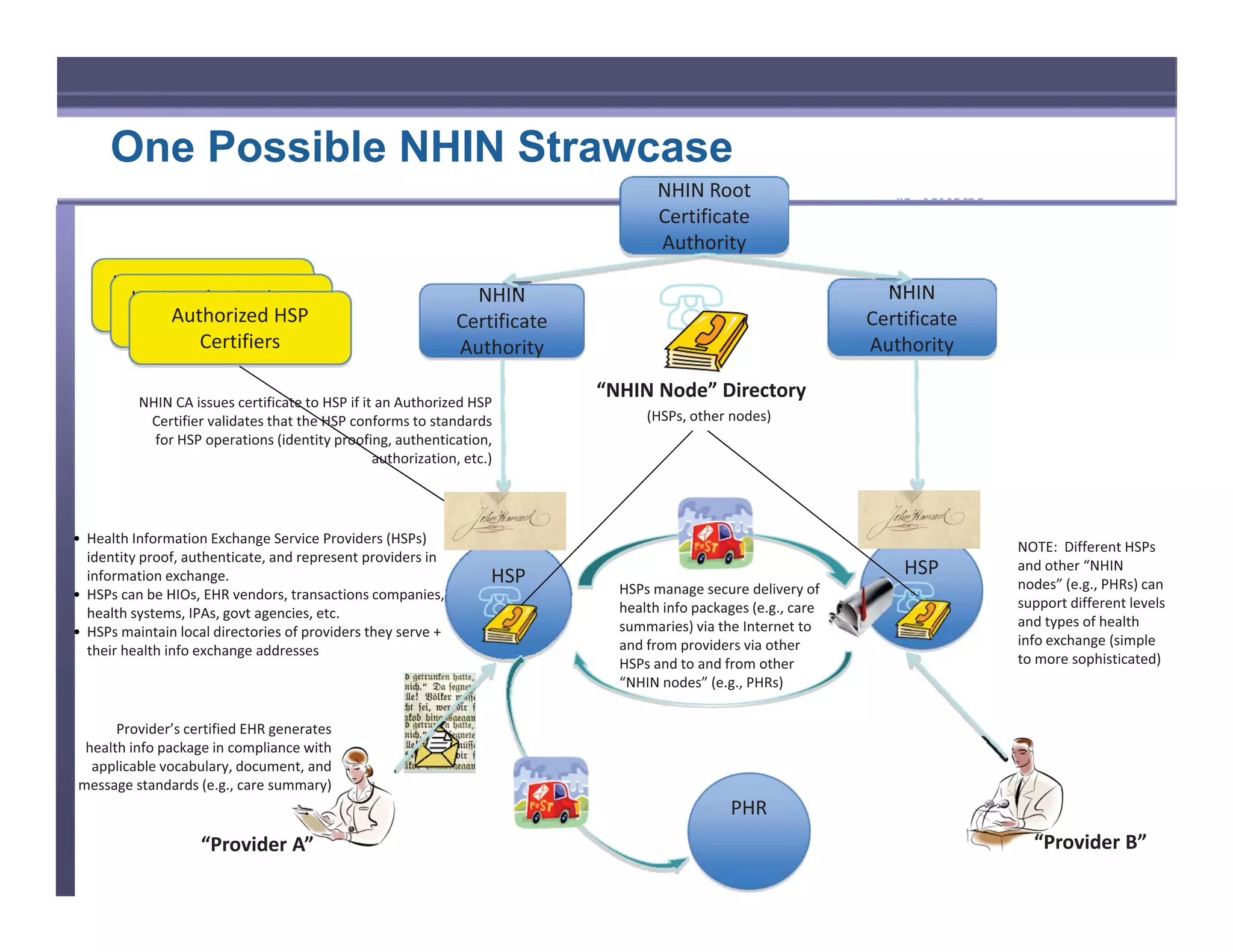

This document summarizes the recommendations of the NHIN Workgroup on enabling health information exchange to support meaningful use requirements. It recommends that the NHIN focus on enabling the broadest provider participation through foundational exchange components like secure internet transport, improved provider directories, and building on existing authentication standards. It also recommends an initial focus on secure information transport rather than data standards, and leveraging existing government provider directories and authentication practices.





















































































