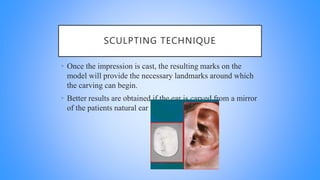
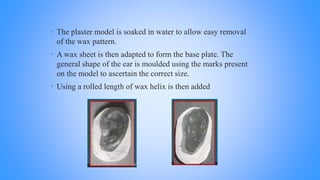
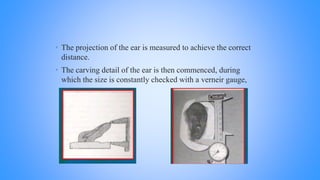
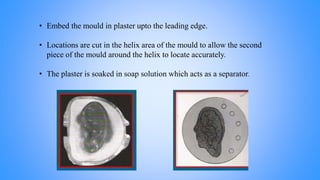
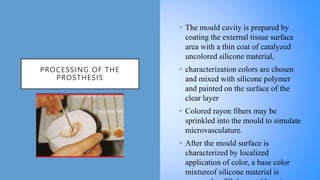
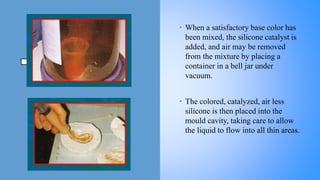
This document discusses the fabrication process of an auricular prosthesis. It begins with definitions of maxillofacial prosthetics and discusses the objectives and advantages/disadvantages of auricular prostheses. It then outlines the full process of fabrication including taking an impression, creating a working cast, sculpting a wax pattern, investing and creating a mold, processing the prosthesis with silicone, applying color, and retaining the prosthesis. The overall goal is to restore esthetics, function, and improve the patient's psychological well-being using prosthetic replacement of missing ear structures.