CONTENTS
• Introduction
• Definition
•Objectives of MFP materials
• Ideal properties of MFP materials
• Factors for successful treatment outcome
• Classification
• Prosthetic reconstruction materials
• Newer materials
• Other products used
• Conclusion
• References
4.
• Maxillofacial prosthesismay be used to treat
or restore tissues of the system and associated
facial structures that have been affected by
disease, injury, surgery or congenital defects.
• Surgical reconstruction is often contraindicated
in the presence of large defects or in high-risk
patients.
• Prosthesis offers the advantage of quick,
reversible and medically uncomplicated
rehabilitation.
5.
• In addition,the restoration may readily be
removed to allow evaluation of the health of
the underlying tissues.
• Maxillofacial prosthetics often "begins where
surgery ends".
6.
DEFINITION
• Maxillofacial prosthetics:the branch of
prosthodontics concerned with the restoration
and/or replacement of stomatognathic and
craniofacial structures with prostheses that may
or may not be removed on a regular or elective
basis.(GPT 9)
• Maxillofacial prosthesis :is defined as any
prosthesis used to replace part or all of any
stomatognathic and/or craniofacial structures.
(GPT 9)
7.
OBJECTIVES OF MAXILLO-FACIAL
PROSTHESES
•Improve the quality of life of patient with
maxillofacial defects.
• Restoration of esthetics or cosmetic
appearance of the patient.
• Restoration of function.
• Psychologic therapy.
• Therapeutic or healing effect.
• Protection of tissues.
8.
Desirable properties ofmaxillofacial
prosthetic material
• Physical properties:-
• The material should be flexible, dimensionally
stable, light in weight, with low thermal
conductivity and good strength.
• Should be flexible at temperatures from 4.4°C to
60°C.
• Biological and Chemical properties:-
• The material should remain stable when exposed
to environmental assaults, adhesives and their
solvents.
9.
• It shouldbe non-toxic, non-allergenic and
biocompatible.
• It should exhibit good life of at least six months
without significant compromise of esthetic and
physical properties.
• Fabrication characteristics:-
• Polymerization should occur at a temperature
low enough to permit reusability of molds.
• Blending of individual components should be
easy, allowing some margin of error. It should
have suitable working time and be easy to color
10.
• Esthetic characteristics:-
•The complete prosthesis should be
unnoticeable in public, faithfully representing
lost structure in the finest detail.
• Its color, texture, form and translucence must
duplicate that of missing structure and adjacent
skin.
• Weight:-
• Light and easily retained in position and be
comfortable to the patient.
11.
Factors for successfultreatment outcome
• Three factors are necessary in evolving a
successful prosthetic facial replacement:-
1. Creative ability
2. Technical knowledge, and
3. Materials which will allow the prosthodontist
to fully exploit these talents.
15.
• The materialsto be evaluated are those, used
in the three phases of the fabrication of the
maxillofacial prosthesis –
1. The impression phase
2. The Modeling phase, and
3. The Fabrication phase
IMPRESSION MATERIALS
• Ideally,impression materials should be able to
reproduce fine detail, be inherently strong, easy
to manipulate, easy to obtain, and
comparatively inexpensive.
18.
REVERSIBLE HYDROCOLLOID- (e.g.AGAR-
AGAR)
ADVANTAGES
1.Reproduces fine detail-records undercuts
2.Easy to manipulate.
3.Easy to obtain.
4.Comparatively inexpensive. (can be reused )
5.Easily applied to patient in upright position,
thereby eliminating smoothing effect of the skin
when the impression is made with the patient in the
reclining position.
19.
• DISADVANTAGES:
1. Requiresrigid backing for sufficient strength
2. Fragility in fine undercut areas
3. Requires two hours of preparation prior to
making the impression
4. Needs intermediary to bond the backing
material
DISADVANTAGES
1. Requires backingfor strength.
2. Fragility in fine undercut areas.
3. Sets slowly at the required consistency ratio
(1 ½ to 1)
4. Requires retaining wall to hold the
impression material in the desired area.
5. Possibility of bubbles, necessitating remakes.
22.
Room Temperature VulcanizingMaterials
ADVANTAGES:
1.Fine detail obtainable
a. Reproduces undercuts
2. Inherent strength
a. Will not tear in fine undercuts
3. Easy to obtain
DISADVANTAGES:
1. Needs backing
2. Difficulty in adjusting setting time
3. Retaining walls needed for confinement of material
4. High cost
23.
Plaster of Paris
ADVANTAGES
1Fine detail obtainable.
2 Inherent strength.
3 Easy to manipulate.
4 Easy to obtain.
5 Low cost.
24.
DISADVANTAGES:
1.Cannot reproduce undercutswithout fracture
a. Easily chipped, with the possibility of
patient aspirating small fragment
2. Exothermic setting reaction of the material
causes discomfort to the exposed mucous
membrane
3. Requires separating medium to prevent
impression from adhering to the model
25.
MODELLING MATERIALS
• Materialsused for modeling should be malleable
to facilitate making gross adjustments to the
contours.
• The material should have sufficient body and
strength to permit sculpting a feather edge and
yet be able to withstand slight abuse.
• It should be possible to sculpt texture into this
material which will be imparted to the finished
mold.
• The closer the color of the material is to the skin
tone, the less visual distortion there will be.
26.
Modeling clay (Sculptor’sClay)
Water-base clay which when allowed to dry, becomes
a hard, stone like substance.
Advantages:
1 Consistency can be adjusted by adding water.
2 Lends itself to gross sculpting of sweeping planes.
3 Takes texture well.
4 Can be feathered on the edge.
5 Inexpensive.
6 Readily available.
27.
Disadvantages:
1 Must bekept moist at all times. If allowed to dry
tends to crack and flake.
2 If the modeling must be set aside for any length
of time the cloth utilized to keep it moist tends to
wipe out the finer texture which has been
incorporated into the model.
3 It is grey in color, and the color differential
causes visual distortion.
28.
Plaster
Advantages:
1 Readily available.
2Inexpensive.
3 Easily and quickly prepared for use.
4 Can be shaped or molded in its plastic state.
Disadvantages:
1 Lacks elasticity.
2 Cannot be used in undercuts.
3 Relatively short setting time.
4 Has a tendency to flake on the surface.
5 Adding material to build contour is difficult.
29.
PLASTOLENE
• A PREPAREDMODELING CLAY WITH OIL BASE/ FULLER’S
EARTH (in india k/a Multani mitti) WITH OIL BASE.
Advantages:
1.Always ready for use.
2.Requires comparatively little care.
3.Can take and keep a feather edge.
4.Easily malleable.
5.Takes texture well.
6.Withstands slight abuse well.
30.
Disadvantages:
1.Color does notmatch the skin.
2.Slightly more expensive than sculptor’s clay.
3.Oil base could seep into stone model and
affect the finished product.
31.
WAXES
ADVANAGES:
1. Color issimilar to skin tone
2. Readily available
3. Nominal cost
4. Withstands abuse
5. Takes and keeps a feather edge
6. Takes texture well
DISADVANTAGES:
7. Model must be carved rather than sculpted
8. Oil base could seep into stone model and affect the
finished product
9. Brittle when cool
32.
UNDERTAKER’S WAXES
It hasalso been used as a modeling wax. The
properties are basically same as those of
standard dental wax, except for two
characteristics
1. because of its low melting point, body heat
will allow it to become malleable , and it can be
then modeled quite readily with fingers and
hands
2. the color is good in relation to skin tissue.
33.
FABRICATION MATERIALS
• Thetype of material employed in making an
extra-oral prosthesis depends to a great extent
upon the prosthodontist’s personal
preference.
• Dentist should pick the material that has the
properties necessary for the successful
treatment of a specific defect.
34.
ACRYLIC RESIN
• Acrylicresins are employed for specific types of
facial defects, particularly those in which little
movement occurs in the tissue bed during
function (e.g. fabrication of orbital prosthesis)
and for temporary facial prostheses.
• Acrylic resin is easily available, easy to stain and
color,has good strength to be fabricated with
feather margin and a good life of about two
years and can be relined or repaired.
37.
Color used:
• Extrinsic– Acrylic base paint used in monomer
or chloroform solvent.
• Intrinsic – Heat polymerized is preferred
compared to auto polymerized because of
reduced residual monomer content, color
stability, free of tertiary amine later.
39.
ACRYLIC CO-POLYMER(PALAMED)
• Acryliccopolymers are soft and elastic but have
not received wide acceptance because of
poor edge strength,
poor durability and
being subject to degradation when exposed to
sunlight
complete restoration is often tacky
predisposing to direct collection and staining.
41.
• Antonucci andStansburry reported the new
generation of acrylic monomers, oligomers
and macromeres.
• They are thermal, chemical and
photointitiated. They can eliminate the short
comings of traditional acrylic co-polymers.
• Plasticizers areadded to produce an elastomeric
effect( rubber like elastic property, flexibility)at
room temperature.
• The primary deficiency arises from migration of
plasticizer leading to discoloration and hardening
of the prosthesis. Absorbs sebaceous secretions,
they compromise the physical properties
• Serviceability not more than 6 months
46.
CHLORINATED POLYETHYLENE
• Lewisand Castleberry reported testing this
material is similar to polyvinyl chloride in both
chemical composition and physical properties.
• Coloration can be done using oil soluble dyes.
• The processing procedure involves high heat
curing with pigmented sheets in metal molds.
47.
• It isless irritating to the mucosa than silicone,
less toxic than thermosetting silicone
materials and non carcinogenic.
• Chlorinated polyethylene elastomer appears
to be a suitable substitute for silicones for the
fabrication of extraoral maxillofacial prosthesis
in situations where cost of silicone is
prohibitive.
48.
Polyurethane elastomers (1970to 1990)
• This material is chemically composed of an
extended segment of aliphatic diisocyanate
groups and a segment of polyol groups (a
mixture of polyesters) and an organotin
catalyst for the polymerization process to
occur.
49.
• Epithane-3 andCalthane are the only
polyurethanes currently available for fabricating
facial prostheses.
• These are 3 component, room-temperature curing
system.
• Part A – Polyol – a combination of polyesters
• Part B – Isocyantate –Mixture of non – yellowing
aliphatic diisocyanates
• Part C – Cartalyst – stannous octate or dibutytin
dilaurate
50.
• Thermosetting deglossingemulsion of
polyurethane elastomer with silica powder to
protect or seal surface colorants.
• These can be used to restore defects with mobile
tissue beds as the positive qualities of this
material pertain to its flexibility without losing
strength at the edges, which allows margins to
be made thin to obtain optimal esthetics.
52.
Silicones
• Barnhart (1960)was the first to use silicone
elastomers for extra-oral prostheses.
• Silicone is a combination of organic and
inorganic compounds and chemically they are
termed as polydimethyl siloxane.
53.
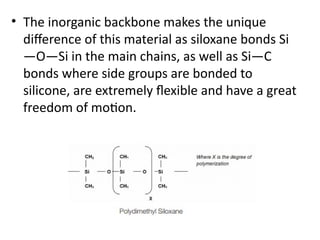
• The inorganicbackbone makes the unique
difference of this material as siloxane bonds Si
—O—Si in the main chains, as well as Si—C
bonds where side groups are bonded to
silicone, are extremely flexible and have a great
freedom of motion.
54.
• This isreflected in their lower viscosity, lower
surface tension, lower melting point and glass
transition temperatures, and is responsible for
the elastomeric behaviors of many
polysiloxanes.
55.
• These becamemore popular over other materials as
they have a range of good physical properties such as
excellent tear and tensile strength over a range of
temperature,
easier to manipulate,
high degree of chemical inertness,
low degree of toxicity, and
high degree of thermal and oxidative stability.
Further they can be stained intrinsically and/or
extrinsically to give them more lifelike natural
appearance.
56.
When adequately cured,silicones elastomers
resist absorbing organic materials that lead to
bacterial growth and so with simple cleaning
these materials are relatively safe and sanitary
compared to other materials
B) Depending ontheir applications:-
•Class I: Implant grade, which requires the material to
undergo extensive testing and must meet “food and
drug administration (FDA)” requirements. These
materials are used in breast implantation.
• Class II: Medical grade, which is approved for
external use.
This material is used for fabrication of maxillofacial
prosthesis.
Some studies tested the cytotoxicity of this material;
however, none has reported any negative side effects.
59.
•Class III: Cleangrade, this material is applied to
use in food coverage and packaging.
• Class IV: Industrial grade, commonly used for
industrial applications.
60.
HTV silicone
• Heat-vulcanizedsilicones are used occasionally
for maxillofacial prostheses.
• It is usually a white, opaque material with a
highly viscous, and putty like consistency.
• It is available as one component or two
component putty.
• The vulcanization mechanism is achieved by
an addition reaction.
61.
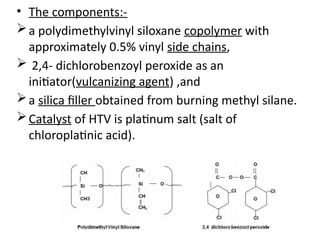
• The components:-
apolydimethylvinyl siloxane copolymer with
approximately 0.5% vinyl side chains,
2,4- dichlorobenzoyl peroxide as an
initiator(vulcanizing agent) ,and
a silica filler obtained from burning methyl silane.
Catalyst of HTV is platinum salt (salt of
chloroplatinic acid).
62.
• The desiredphysical and mechanical properties
can be achieved by altering the ratio of the matrix
and the filler particles.
• Addition of opaque fillers increases strength but
can compromise with translucency of prosthesis.
• Vulcanization/ cross linking is by free radical (of
organic peroxide) addition polymerization (so no
by product), which results from thermal
decomposition of the initiator to form free
radicals that cross-link the copolymer into a three
dimensional resilient structure
63.
• The processingtemperature is 180°C- 220°C for
about 30 min under pressure using metal molds.
• The copolymer is supplied as a rubbery solid with
a high viscosity.
• The pigments are incorporated into the polymer
with roller mills.
• Although this material is more difficult to pigment
and process, excellent results can be obtained.
64.
• Advantages:-
- Excellenttear strength and highest tensile strength
at 5.87 MPa (polyurethane the lowest at 0.83 MPa.).
- Excellent thermal, colour and chemical stability
(rendering it more biologically inert).
- High percent elongation.
• Disadvantages:-
- Poor esthetics due to opacity.
- Less elasticity.
- Low edge strength.
- Technique sensitive.
65.
• VARIOUS TYPESOF HTV SILICONES:
• Silastic S-6508, 382 and 399 (Michigan)
• Silastic S-6508 is in raw state which is similar to
sticky modeling clay. It must be vulcanized at
250OF and formed in pressure molds.
• Silastic 382 is an opaque white fluid with a
viscosity like that of a thick honey.
• Silastic 399 resembles white vaseline in its raw
state. Easily spatulated, but non-flowing.
• Silastic 382, tougher non-flowing, but easier to
handle.
66.
RTV silicone (Roomtemperature vulcanizing)
• There are two types:
1. Cross linking by condensation reaction:
• They have reactive groups such as silariols
(hydroxyl- terminated polysiloxanes).
• a cross linking agent, eg. tetraethyl silicate,
and
• a catalyst, e.g. dibutyltin dilaurate
67.
Examples
• Medical AdhesiveType A (Dow Corning), where
methyl triacetoxy silane (II) is used as the cross-
linking agent.
• The cross-linking, however, requires water
molecules to hydrolyze the silane and produces
acetic acid (an irritant) as the by-product.
• The use has therefore been limited to that of an
extrinsic colourant carrier applied to the surface
of the prosthesis.
68.
• Disadvantages:-
- Producesby- products.
- Curing time is excessively long making it
impractical for curing the material inside a mold.
- Degradation reactions such as hydrolysis.
- Relatively low tear strength and are incapable
of maintaining edge resistance
69.
2. Cross-linking ofpolysiloxanes by addition
reactions
• The reactions generally involve the addition of
silyl hydride groups (—SiH) to vinyl groups
(CH2=CH—) attached to the silicone with the aid
of a platinum containing catalyst.
• These silicones are not truly room vulcanized
silicones.
• The curing of these silicones, in fact, requires
heating the material at 150°C for a time, possibly
an hour.
70.
• These materialshave improved tear strength over
the first type of RTV silicones.
• Disadvantages:-
- Very hydrophobic.
- Selective adhesive property.
- No extrinsic colouration.
- Cure of the materials may be inhibited by traces of
amines, sulfur, nitrogen oxides and organo-tin
compounds.
71.
• Room-temperature-curing siliconesare supplied
as single-component materials that cure by
evaporation of acetic acid.
• They are characterized by a natural flesh-like
appearance by using dyed rayon fibers, dry earth
pigments, and/or oil paints.
• Prostheses are polymerized by bulk multiple
packing.
• Recently epoxy resins and stainless steel molds
are being used.
72.
• Advantages ofthe RTV silicone material-
use of stone molds,
ease of manipulation
ease of colouring,
colour stability and
biological inertness.
73.
• Examples: Silastic382, 399, 891, MDX4-4210,
Cosmesil, A-2186, and A-2186F.
• MDX4-4210, a clear-to-translucent two part (10:1,
base: catalyst) silicone was introduced to the
maxillofacial prosthetics field in the 1970s
• It includes Filler - Silica / Diaatomaceous earth
particles
• catalys - Chloro platanic acid
• Cross liking agent - Hydro-methyl siloxane
• Polymerization – additional silicon
74.
• Factor II(Lakeside, AZ), introduce in 1986
A- 2186 was the first commercial platinum-
catalyzed silicone elastomer.
• It is a clear-to-translucent two-part (10:1
base:catalyst) pourable silicone.
• A fast polymerization rate version of A-2186
with higher platinum content, “A-2186F,”
became commercially available in 1987.
• It was not a very preferred material for
prosthesis purpose.
75.
• In 2000,Factor II introduced A-2000 as the first
generation of a 1:1mixture platinum silicone
followed by A-2006 in 2006.
• Several other commercially available silicone
products have been introduced since 1992,
including Cosmesil, Realastic, VerSil- Tal (VST),
and Liquid Silicone Rubber (LSR) Systems to
name a few.
76.
ADVANTAGES OF HTVOVER RTV
• Less chances of air bubble entrapment,since
hand mixing of catalyst and pigments with the
elastomer is avoided.
• Increased tear strength, mechanical durability,
and chemical resistance.
• Increased biocompatibility and flexibility.
• BASIC DIFFERENCE BETWEEN HTV AND RTV IS
THAT HTV IS NOT AS ELASTIC AS RTV THEREFORE
NOT SUITABLE FOR MOBILE TISSUE BEDS
77.
• The expectedhalf-life of maxillofacial
prosthesis is approximately six months and
degradation of physical and colour properties
of silicones are the most common reasons for
re-fabrication.
78.
NEWER MATERIALS
• Foamingsilicones:
• Silastic 386 – in it is a type of RTV material.
• The basic silicone has an additive which
release gas when the catalyst (stannous
octoate) is introduced.
• The purpose of the foam forming silicones is
to reduce the weight of the prosthesis
79.
• Major disadvantageof foamed material is
reduced strength and is susceptible to
straining, leading to weakening of the
material.
• This weakness can be overcome partially by
coating foam with another silicone which adds
strength but increase stiffness
80.
• Siphenylenes:
• Theseare siloxane copolymers that contain
methyl and phenyl groups.
• These exhibit improved edge strength, low
modulus of elasticity and colour stability over
the more conventional polydimethyl siloxane
81.
• Silicone BlockCopolymers: In this blocks of polymers
other than siloxane are positioned with the
traditional siloxane polymers.
• The hydrophobic nature and foreign nature of
silicones has been proven to cause problems,
especially with regard to the interaction with the
body on a molecular level.
• This can lead to the induction of foreign body
reactions and the development of infections
particularly at the interface between silicone and
tissue.
82.
• These siliconeblock copolymers can to some
extent overcome these problems as the more
hydrophilic part of these amphiphilic polymers
provides improved wettability and thus tissue
compatibility.
• An example of this is the intertwining of poly
methyl methacrylate into the chains of siloxane
83.
• Polyphosphazenes:
• Researchershave found that compounding
Polyphosphazenes with little or no fillers and
decreasing the ratio of acrylic to rubber yields a
softer rubber similar to human skin.
• The rubber is compounded with pigments for
appropriate matching with the patients’ skin
84.
Other products used
•Primer
• With the introduction of urethane-line silicone
prosthesis, there has been an increased interest
in primers used for promotion of bonding
between silicone and other maxillofacial
prosthetic material 1200, 1205, S-2260, 4040,
Z6032 and Z 607.
85.
Adhesives
• A varietyof adhesive systems have been employed to
retain facial prostheses in position. They are commonly
classified by the method in which they are dispensed:
Parts, liquid, emulsions, sprayers and double sided
tapes. Double sided tape is the most commonly used
(41%) among patients with facial prostheses because
of its ease of application, removal and maintenance.
Most cured silicones, because of their low solubility
and low surface energy, will not adhere to
conventional tissue adhesive. The single component
RTV silicones were developed to serve as adhesives for
silicon prostheses (Medical Adhesive Type A).
86.
• Colours-
• Thereare intrinsic and extrinsic methods of
colouring.
INTRINSIC COLOUR:-
Dry earth pigments, rayon flocking fibers (most
commonly used), artist’s oil pigments, or a
combination of these materials for intrinsic tinting.
Kaolin material was commonly used as an opacifier.
88.
• EXTRINSIC COLOUR:-
The most-used extrinsic colouring method was Medical Adhesive Type-A
mixed with Xylene as a retarder/thinner tinted with dry earth pigments or
artist’s oil pigments applied to the surface of the prosthesis in a thin
layer.
CONCLUSION
• When reviewingthe advantages and
disadvantages of each of these materials, it is
obvious that no single material is ideal for every
patient.
• Some of the problems inherent in all these
materials are:
1. The continued effect of sunlight and vascular
dilation and contraction on the natural tissues,
which cannot be duplicated in the prosthesis.
94.
2.The variations ofskin tone when the patient is
exposed to different light sources (e.g.,
incandescent, fluorescent, and natural light).
3. Emotional factors which cause color changes in
the skin.
4. The inability of the prosthesis to duplicate the
full facial movement of the nondefective side.
5. Lack of predictability of the life of the
prosthesis, because of the variations among the
patients (i.e., secretions, smoking and
environment).