2. Key Points
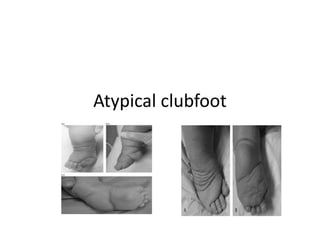
• Atypical clubfeet have
– severe equinus
– plantarflexion of all metatarsals
– a short hyperextended great toe
• Atypical clubfeet are challenging to treat
• Initial treatment with the modified Ponseti method
can be successful, but relapses and complications are
frequent
3. Description
• Atypical clubfeet or complex
idiopathic clubfeet are defined
by Ponseti as
– having rigid equinus
– severe plantar flexion of all
metatarsals
– a deep crease above the
heel
– a transverse crease in the
sole of the foot
– a short hyperextended first
toe
4. • While typical idiopathic clubfeet respond well to the standard
method of Ponseti casting and generally correct after 4-6
casts, atypical clubfeet are resistant to correction and
standard manipulation and casting may lead to worsened
deformity.
• They respond differently to operative and nonoperative
treatment.
• Early surgery can result in a grotesquely deformed foot
(Ponseti, 2006).
• While they may also be difficult to treat, arthrogrypotic,
syndromic, and neuromuscular clubfeet are excluded from the
definition of atypical or complex idiopathic clubfeet.
5. Epidemiology
• A small percentage of idiopathic clubfeet are
classified as atypical.
• In Ponseti’s series 6.5% of idiopathic clubfeet
were atypical and 68% of these occurred in
boys. (Ponseti, 2006)
6. Clinical findings
• Significant shortening
• Increased creases
• Rigid equinus with a deep crease above the heel
• Severe plantar flexion of all metatarsals with a deep
plantar crease across the full width of the sole of the foot
• High cavus
• Short and hyperextended big toe
• Normal neurologic examination.
7. • The Achilles tendon is long and wide with the gastrocsoleus muscle
bunched in the proximal third of the calf.
• The anterior calcaneus is prominent dorsolaterally and in contact with the
small and often difficult to palpate talar head.
• The navicular is displaced medially contacting the medial malleolus.
• Two-thirds of patients with atypical clubfeet demonstrate anterolateral
bowing of the tibia, and there is a greater size discrepancy in unilateral
atypical clubfoot compared to the unaffected contralateral foot than is
usually seen in unilateral idiopathic clubfoot.
8. *Significant shortening *Increased creases
*High cavus *Short and hyperextended big toe
*Rigid equinus with a deep crease above the heel
*Severe plantar flexion of all metatarsals with a deep plantar crease across the full
width of the sole of the foot
9. Xrays
• The talocalcaneal angle is generally parallel on both the
AP and lateral views.
• The cuboid is displaced medially.
• There is severe plantarflexion of the talus, calcaneus,
and all metatarsals, especially the first metatarsal.
• In patients who have developed abduction of the
forefoot after attempted casting, the metatarsals may
be hyperabducted at the tarsal-metatarsal joins with
up to 90 degrees of plantarflexion.
10.
11.
12. Etiology
• Ponseti attributed the cause of atypical clubfeet to the very shortened and
fibrotic tendoachilles, contracted deep plantar intrinsic muscles, and tight
ligaments within the foot.
• Improper casting has been suggested as a contributing factor (Matar,
2017).
• This pathoanatomy allows the forefoot adduction to be easily corrected
with casts, but causes the metatarsals to remain in severe plantarflexion.
– Continued attempts at abduction push the metatarsals into additional flexion
and abduction but do not correct the hindfoot varus as the intrinics are
unyielding (Ponseti, 2006).
• An accessory muscle, the flexor digitorum accessorius longus, has been
described as a muscle belly crossing over the neurovascular bundle medial
to the Achilles with its tendon running alongside flexor hallucis longus and
inserting on only two of the lateral 4 toes.
– This correlated with the clinical finding of an extended great toe in 95.8% of
cases and was suggested to contribute to the flexed posture of the lesser toes
in relation to the hallux (Shaheena, 2015).
13. • Patients with complex idiopathic clubfeet and peroneal nerve
dysfunction noted prior to or after treatment have been
reported. Interestingly, these patients were noted to have the
drop toe sign rather than the hyperextended great toe
(Morcuende, 2010).
• Soft tissue abnormalities including excess epimysial fat,
intramuscular fat replacement, and decreased muscle area
have been found in treatment-resistant clubfeet that
experienced relapse when compared to treatment-responsive
clubfeet.
• Hypoplasia in specific muscle groups was also noted in a
subset of patients.
14. Treatment
• Modified Ponseti method
– An effective first line treatment for atypical
clubfoot.
– Requires an increased number of casts and an
increased rate of relapse and surgical releases
have been reported (Matar, 2017).
– Higher rates of relapse and risk factors for relapse
of the more severe clubfoot have been identified
(Sangiorgio 2017).
15. The subtalar joint and head of the talus must be
precisely identified, which may be difficult due to the
prominent anterior process of the calcaneus
Once identified, place the thumb over the talar head and
index finger on the posterior aspect of the lateral
malleolus and then gently abduct the foot with the other
hand. Care should be taken not to over abduct the
forefoot.
Once the forefoot abduction is corrected, the
plantarflexion of all metatarsals is addressed by grasping
the ankle with both hands and dorsiflexing the foot with
both thumbs while an assistant supports the knee in
flexion. The knee should be casted in at least 110
degrees of flexion to prevent cast slippage.
16. Percutaneous Achilles tenotomy is performed after
plantarflexion of the metatarsals has been
corrected. The site chosen is 1.5cm above the posterior
skin crease as opposed to the traditional 1cm to avoid
injury to the proximally positioned posterior tuberosity
of the calcaneus.
A second Achilles tenotomy may be required for some
patients with serial casting following until five degrees of
dorsiflexion and no more than 40 degrees of abduction
are obtained.
At this point abduction bracing is initiated with a soft 3-
strap sandal attached to the bar at 40 degrees of
external rotation (Ponseti, 2006).
17. Complications
• Atypical clubfeet do not correct with the standard Ponseti method.
• Frequent cast slipping may cause foot edema, bruising, and skin
breakdown.
• Ponseti reported a 22% complication rate with his modified method
including erythema, swelling of the forefoot and toes, mild rocker-bottom
deformity, midfoot hyperabduction, and repeated downward cast
slippage.
• Relapse rate at 2 years was 14%, and most frequently attributed to
difficulty with ill-fitting shoes during abduction bracing (Ponseti, 2006).
• Using the modified Ponseti method, Matar found 53% relapse at 7 years
average follow up (range 3-11 years) (Matar, 2017).