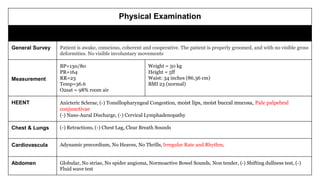
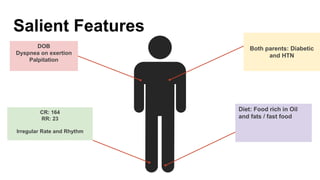
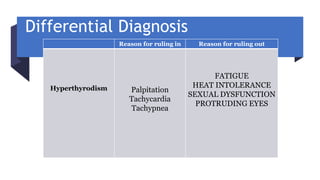
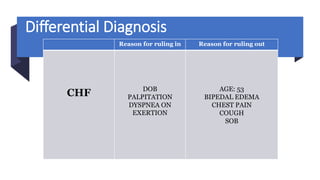
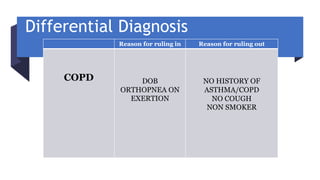
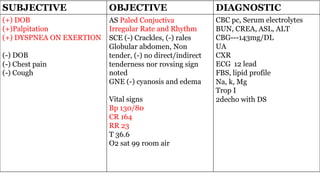
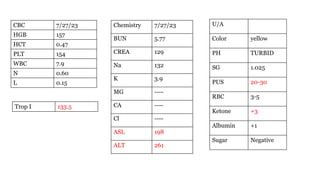
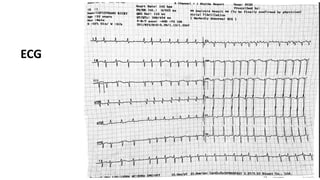
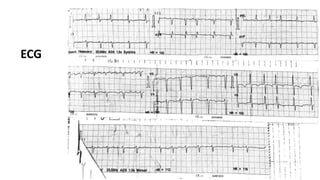
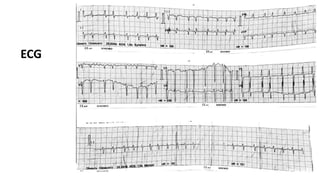
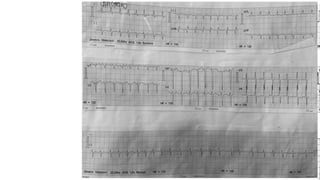
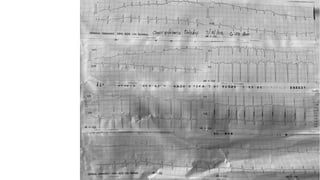
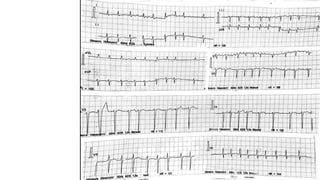
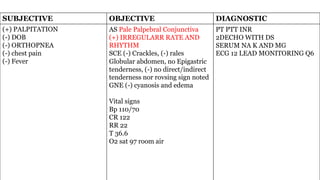
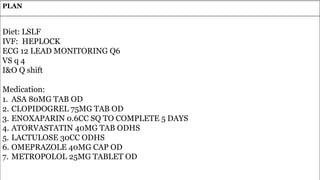
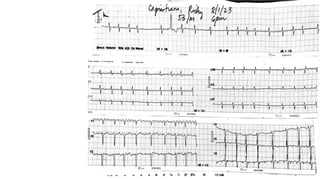
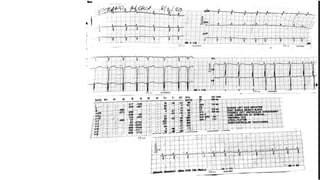
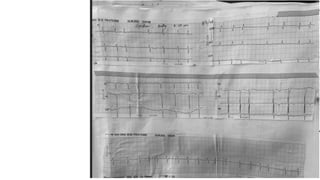
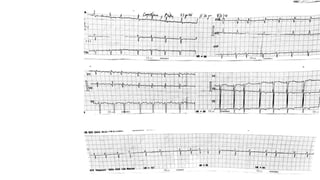
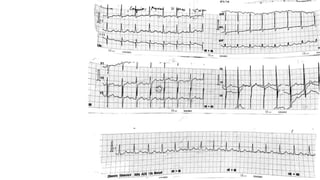
The document presents a case study of a 53-year-old male patient who presented with difficulty breathing, palpitations, and dyspnea on exertion. Upon examination, the patient was found to have an irregular heart rate and rhythm consistent with atrial fibrillation. Differential diagnoses included hyperthyroidism, CHF, and COPD, but these were ruled out based on the patient's history and examination findings. The working diagnosis was atrial fibrillation in rapid ventricular response.