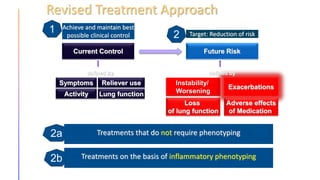
The document discusses asthma management guidelines and provides several case scenarios. It covers investigations for initial asthma evaluation including CBC, IgE, chest X-ray, and echocardiogram. It discusses asthma mimics, comorbidities, inhaler selection, exacerbation risk factors including viral infections, and the importance of preventing exacerbations to reduce healthcare costs and lung function decline. It also notes that referral to a dedicated asthma clinic is important.


![ADVANCED LAB / IMMUNOLOGICAL TESTING
• For patients with severe persistent asthma, a CBC and differential (to evaluate
the presence/absence of eosinophils and exclude anemia as a cause of
dyspnea) and a total serum immunoglobulin E (IgE) level (eg, for allergic
bronchopulmonary aspergillosis [ABPA] or for identification of candidates for
anti-IgE therapy) are usually obtained.
• Specific testing for aspergillus sensitization (skin test or immunoassay) and an
antineutrophil cytoplasmic antibody (ANCA) are performed in those with high
blood eosinophils to evaluate for ABPA and eosinophilic granulomatosis with
polyangiitis (EGPA, Churg-Strauss), respectively](https://image.slidesharecdn.com/asthmamanagementandgina-221028191138-69ade6a2/85/Asthma-management-and-GINA-pptx-14-320.jpg)




















![Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency - CASE STUDY [pediatrics]](https://cdn.slidesharecdn.com/ss_thumbnails/g6pd-180215232015-thumbnail.jpg?width=640&height=640&fit=bounds)





































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)















