MEDICINE
MEDICINE
ASTHMA
ASTHMA
PRESENTER : MRSANGWILE
PRESENTER : MR SANGWILE
BACHELOR’S OF NURSING
BACHELOR’S OF NURSING
MASTERS IN PUBLIC HEALTH NURSING
MASTERS IN PUBLIC HEALTH NURSING
2.
General Objective
General Objective
At the end of this lecture/discussion,
At the end of this lecture/discussion,
students should acquire knowledge on
students should acquire knowledge on
Broncho Asthma and be able to nurse
Broncho Asthma and be able to nurse
patients with this condition.
patients with this condition.
3.
Specific Objectives
Specific Objectives
At the end of the lecture/discussion students
At the end of the lecture/discussion students
should be able to:
should be able to:
1.
1. Define Asthma.
Define Asthma.
2.
2. State the classification of Asthma.
State the classification of Asthma.
3.
3. Mention the predisposing factors of
Mention the predisposing factors of
Asthma.
Asthma.
4.
Specific Objectives
Specific Objectives
4. Describe the Pathophysiology of Asthma.
4. Describe the Pathophysiology of Asthma.
5.
5. State the signs and symptoms of
State the signs and symptoms of
Asthma.
Asthma.
6.
6. Outline the Medical management of
Outline the Medical management of
Asthma.
Asthma.
5.
Specific Objectives
Specific Objectives
7.
7. Discuss the Nursing Care rendered to
Discuss the Nursing Care rendered to
an Asthmatic Patient.
an Asthmatic Patient.
8.
8. Elaborate the Information, Education
Elaborate the Information, Education
and Communication (I.E.C) you can give in
and Communication (I.E.C) you can give in
Asthma.
Asthma.
9.
9. State the complications of Asthma.
State the complications of Asthma.
Definition
Definition
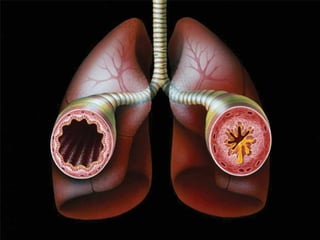
A) It isa common chronic inflammatory
A) It is a common chronic inflammatory
condition of the airways characterised by
condition of the airways characterised by
reversible airflow obstruction and
reversible airflow obstruction and
bronchospasms, severe dyspnea, wheezing,
bronchospasms, severe dyspnea, wheezing,
chest tightness and expiratory exertion
chest tightness and expiratory exertion
(Stellenberg 2007).
(Stellenberg 2007).
9.
Definition
Definition
B) Itis a respiratory disorder characterised
B) It is a respiratory disorder characterised
by recurrent attacks of dyspnea, wheezing
by recurrent attacks of dyspnea, wheezing
and coughing due to hyperactive airway
and coughing due to hyperactive airway
resulting in mucosal swelling, broncho
resulting in mucosal swelling, broncho
constriction and increased secretion of
constriction and increased secretion of
mucus.
mucus.
10.
TYPES OF ASTHMA
TYPESOF ASTHMA
Extrinsic Asthma is also called Allergic
Extrinsic Asthma is also called Allergic
Asthma (atopic) because patients are
Asthma (atopic) because patients are
allergic to a wide range of allergens. This is
allergic to a wide range of allergens. This is
the commonest type accounting for about 90
the commonest type accounting for about 90
% of all cases. It occurs in individuals who
% of all cases. It occurs in individuals who
have already formed immuno globulin E
have already formed immuno globulin E
(IgE) antibodies to common Allergens such
(IgE) antibodies to common Allergens such
as pollen.
as pollen.
11.
TYPES OF ASTHMA
TYPESOF ASTHMA
Intrinsic Asthma is not usually associated
Intrinsic Asthma is not usually associated
with any allergies (non atopic) and accounts
with any allergies (non atopic) and accounts
for about 10% of the cases. It starts later in
for about 10% of the cases. It starts later in
life usually after the age of 30.
life usually after the age of 30.
12.
PREDISPOSING FACTORS
PREDISPOSING FACTORS
TheCause of Asthma is Idiopathic, however, the
The Cause of Asthma is Idiopathic, however, the
are several predisposing factors
are several predisposing factors
•
•Allergen inhalation:
Allergen inhalation:
•
•Environmental factors
Environmental factors
•Prolonged exposure to cold.
Prolonged exposure to cold.
13.
PREDISPOSING FACTORS
PREDISPOSING FACTORS
•
•Medications:such as Asprin and Ibuprofen
Medications: such as Asprin and Ibuprofen
•
•Atmospheric pollutants: Cigarette and industrial
Atmospheric pollutants: Cigarette and industrial
smoke, sulphur dioxide, wood smoke, exhaust
smoke, sulphur dioxide, wood smoke, exhaust
fumes
fumes
•
•Psychological Factors: Stress/emotional upset
Psychological Factors: Stress/emotional upset
coupled with crying and shouting
coupled with crying and shouting
14.
PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
•
•Exposure to anallergy such as Pollen or
Exposure to an allergy such as Pollen or
cigarette smoke for the first time will triggers the
cigarette smoke for the first time will triggers the
immune response to produce immuno globulin E
immune response to produce immuno globulin E
(IgE) in large amounts.
(IgE) in large amounts.
•
•Further exposure to this allergen will lead to an
Further exposure to this allergen will lead to an
antigen antibody reaction.
antigen antibody reaction.
15.
PATHOPHYSIOLOGY cont…
PATHOPHYSIOLOGY cont…
This will be followed by the release of histamine
This will be followed by the release of histamine
from the mast cells to the site of irritation, in this
from the mast cells to the site of irritation, in this
case the walls of the airways.
case the walls of the airways.
Histamine is an inflammatory mediator which
Histamine is an inflammatory mediator which
triggers an inflammatory response.
triggers an inflammatory response.
16.
PATHOPHYSIOLOGY cont…
PATHOPHYSIOLOGY cont…
•
•Thisinflammatory response causes
This inflammatory response causes
bronchospasms, in which the muscles lining the
bronchospasms, in which the muscles lining the
airways contract repeatedly, causing broncho
airways contract repeatedly, causing broncho
constriction.
constriction.
•
•There is also vascular congestion, oedema
There is also vascular congestion, oedema
formation, thickening of the airway walls and
formation, thickening of the airway walls and
increased bronchial hyper-responsiveness
increased bronchial hyper-responsiveness
17.
Pathophysiology cont….
Pathophysiology cont….
Gobletcells which produce mucus become
Goblet cells which produce mucus become
hyperactive due to inflammatory response and
hyperactive due to inflammatory response and
secrete thick tenacious mucus in excess.
secrete thick tenacious mucus in excess.
This mucus clogs the bronchioles further
This mucus clogs the bronchioles further
impairing the airflow, resulting in wheezing and
impairing the airflow, resulting in wheezing and
coughing.
coughing.
18.
Pathophysiology cont
Pathophysiology cont
The inflammation of the broncho mucosa
The inflammation of the broncho mucosa
narrows the airway causing difficulties in
narrows the airway causing difficulties in
breathing.
breathing.
•
•The obstruction of air flow causes impaired
The obstruction of air flow causes impaired
alveolar ventilation causing Dyspnea and
alveolar ventilation causing Dyspnea and
trapping air in the lungs.
trapping air in the lungs.
19.
Pathophysiology cont
Pathophysiology cont
•
•Inorder to expel air from the lung expirations
In order to expel air from the lung expirations
are forced and accessory muscles of
are forced and accessory muscles of
respiration are brought into action causing
respiration are brought into action causing
intercoastal retractions.
intercoastal retractions.
20.
Pathophysiology cont
Pathophysiology cont
The result is intense inflammatory response
The result is intense inflammatory response
in the airways, impaired muco-ciliary
in the airways, impaired muco-ciliary
function and altered gaseous exchange.
function and altered gaseous exchange.
If not treated, the condition can lead to
If not treated, the condition can lead to
respiratory failure.
respiratory failure.
22.
sign and symptomscontinue
sign and symptoms continue
Dyspnea due to impaired ventilation
Dyspnea due to impaired ventilation
Wheezing as air passes through a fluid filled and
Wheezing as air passes through a fluid filled and
constricted airway
constricted airway
Coughing with or without sputum as an attempt
Coughing with or without sputum as an attempt
to clear the air way of the secretions and irritants.
to clear the air way of the secretions and irritants.
23.
sign and symptomscontinue
sign and symptoms continue
•
• Anxiety and restlessness due to shortness of
Anxiety and restlessness due to shortness of
breath
breath
•
• Cyanosis due to hypoxia
Cyanosis due to hypoxia
•
• Nasal flaring due to dyspnea and insufficient air
Nasal flaring due to dyspnea and insufficient air
entry.
entry.
24.
sign and symptomscontinue
sign and symptoms continue
• Profuse sweating due to labored breathing,
Profuse sweating due to labored breathing,
increased metabolic rate and anxiety.
increased metabolic rate and anxiety.
•
• Intercostal retraction due to involvement of
Intercostal retraction due to involvement of
accessory muscles of respiration.
accessory muscles of respiration.
25.
sign and symptomscontinue
sign and symptoms continue
Tightness in the chest due to pressure build up
Tightness in the chest due to pressure build up
caused by broncho occlusion
caused by broncho occlusion
Drowsiness or confusion due to cerebral
Drowsiness or confusion due to cerebral
hypoxia
hypoxia
26.
INVESTIGATIONS
INVESTIGATIONS
*History will reveal:
*History will reveal :
Cough, worse particularly at night
Cough, worse particularly at night
Recurrent wheezing
Recurrent wheezing
Recurrent difficulty in breathing
Recurrent difficulty in breathing
Recurrent chest tightness
Recurrent chest tightness
27.
INVESTIGATIONS
INVESTIGATIONS
*Physical examinations:
*Physical examinations:
Inspectionwill reveal intercoastal retractions.
Inspection will reveal intercoastal retractions.
Audible wheezing or wheezing heard on
Audible wheezing or wheezing heard on
Auscultation.
Auscultation.
*Full Blood Count (FBC) will reveal elevated
*Full Blood Count (FBC) will reveal elevated
eosinophil count, and elevated IgE levels.
eosinophil count, and elevated IgE levels.
28.
INVESTIGATIONS
INVESTIGATIONS
*Arterial blood studieswill show elevated levels of
*Arterial blood studies will show elevated levels of
carbon dioxide and reduced Partial pressure of
carbon dioxide and reduced Partial pressure of
oxygen.
oxygen.
*Chest X ray to rule out chest infection.
*Chest X ray to rule out chest infection.
It can also show hyperinflation of the lung
It can also show hyperinflation of the lung
tissue.
tissue.
29.
TREATMENT
TREATMENT
1.BRONCHIAL DILATORS:
1.BRONCHIAL DILATORS:
Bronchodilatorsstimulate beta adrenergic
Bronchodilators stimulate beta adrenergic
receptors to relax the bronchial muscles and
receptors to relax the bronchial muscles and
widen the airways.
widen the airways.
Aminophylline IV: 250mg/10mls Ampoule
Aminophylline IV: 250mg/10mls Ampoule
Aminophylline tab: 100mg-200mg Per oral
Aminophylline tab: 100mg-200mg Per oral
TDS
TDS
Epinephrine (Adrenalin) 0.5mg/ml
Epinephrine(Adrenalin) 0.5mg/ml
0.5mls subcutaneously or intramuscularly
0.5mls subcutaneously or intramuscularly
repeated after 10-15minutes, PRN
repeated after 10-15minutes, PRN
S/E: Nervousness, tremors, headache,
S/E: Nervousness, tremors, headache,
palpitations, cerebral haemorrhage and
palpitations, cerebral haemorrhage and
dyspnoea.
dyspnoea.
32.
OXYGEN THERAPY
OXYGEN THERAPY
Humidifiedoxygen is given to ease breathing and
Humidified oxygen is given to ease breathing and
improve tissue perfusion.
improve tissue perfusion.
Administer 4-6litres/minute in adults, by nasal
Administer 4-6litres/minute in adults, by nasal
catheter or face mask.
catheter or face mask.
33.
ANALGESICS FOR PAINRELIEF
ANALGESICS FOR PAIN RELIEF
Paracetamol 500-1000mg tds for 3days.
Paracetamol 500-1000mg tds for 3days.
ANTIBIOTIC THERAPY
ANTIBIOTIC THERAPY
Given to combat infection, if cause of an
Given to combat infection, if cause of an
asthmatic attack is due to infections like
asthmatic attack is due to infections like
bronchitis.
bronchitis.
COMPLICATION
COMPLICATION
Pneumothorax; dueto trapped air in the lungs.
Pneumothorax; due to trapped air in the lungs.
Pneumonia; due to accumulation of thick
Pneumonia; due to accumulation of thick
tenacious mucus and the overall inflammatory
tenacious mucus and the overall inflammatory
process.
process.
36.
COMPLICATION
COMPLICATION
Emphysema; achronic lung condition
Emphysema; a chronic lung condition
characterised by alveolar enlargement,
characterised by alveolar enlargement,
dilatation and lack of flexibility thereby
dilatation and lack of flexibility thereby
impairing breathing.
impairing breathing.
37.
COMPLICATION
COMPLICATION
Atelectasis; Partialor total collapse of the lung
Atelectasis; Partial or total collapse of the lung
tissue.
tissue.
Respiratory distress; due to exhaustion and
Respiratory distress; due to exhaustion and
hypoxia
hypoxia
Cardiac arrest; due to pulmonary oedema
Cardiac arrest; due to pulmonary oedema
which exerts undue pressure on the heart.
which exerts undue pressure on the heart.
38.
COMPLICATION
COMPLICATION
Status Asthmaticus;is a long lasting and
Status Asthmaticus; is a long lasting and
severe asthmatic attack that does not respond
severe asthmatic attack that does not respond
to standard treatment and places the patient at
to standard treatment and places the patient at
risk of developing respiratory failure.
risk of developing respiratory failure.
39.
ASSIGNMENT
ASSIGNMENT
Go andread on the management of Status
Go and read on the management of Status
Asthmaticus
Asthmaticus
40.
NURSING CARE FORASTHMATIC
NURSING CARE FOR ASTHMATIC
PATIENT
PATIENT
AIMS
AIMS
To relieve dyspnea
To relieve dyspnea
To alley anxiety
To alley anxiety
To promote quick recovery
To promote quick recovery
To prevent complications
To prevent complications
To maintain tissue perfusion
To maintain tissue perfusion
41.
ENVIRONMENT
ENVIRONMENT
Patient willbe nursed:
Patient will be nursed:
.at the acute bay for close observation
.at the acute bay for close observation
.in a well-ventilated room to promote oxygen
.in a well-ventilated room to promote oxygen
and prevent other respiratory tract infections.
and prevent other respiratory tract infections.
. in a well lit room for easy observation.
. in a well lit room for easy observation.
42.
. under barriernursing to prevent him from
. under barrier nursing to prevent him from
acquiring of nosocomial infections.
acquiring of nosocomial infections.
Position
Position
•
• Patient will be nursed in propped up position to
Patient will be nursed in propped up position to
promote lung expansion and relieve dyspnea
promote lung expansion and relieve dyspnea
43.
Rest
Rest
I will:
I will:
administeroxygen as the condition demands to
administer oxygen as the condition demands to
promote ventilation.
promote ventilation.
nurse the patient in a quiet room to promote
nurse the patient in a quiet room to promote
rest.
rest.
do related procedures in blocks to promote rest.
do related procedures in blocks to promote rest.
44.
observations
observations
TPR andBP will help me to know if the
TPR and BP will help me to know if the
condition is improving or deteriorating.
condition is improving or deteriorating.
Respirations are likely to be slow and deep and
Respirations are likely to be slow and deep and
this will help me to detect any deviations from
this will help me to detect any deviations from
normal.
normal.
observe for cyanosis and give oxygen therapy
observe for cyanosis and give oxygen therapy
when necessary.
when necessary.
45.
Observations cont…
Observations cont…
I will observe Dyspnea, if present, i will prop up
I will observe Dyspnea, if present, i will prop up
the patient to promote lung expansion and
the patient to promote lung expansion and
there by relieving dyspnea.
there by relieving dyspnea.
I will observe the sputum for colour amount and
I will observe the sputum for colour amount and
consistency to detect haemoptysis and report
consistency to detect haemoptysis and report
the physician.
the physician.
46.
Psychological Support
Psychological Support
As a nurse, I will maintain a calm and
As a nurse, I will maintain a calm and
reassuring manner.
reassuring manner.
I will explain the disease process in order to
I will explain the disease process in order to
raise the knowledge levels and thereby alley
raise the knowledge levels and thereby alley
anxiety.
anxiety.
I will explain all procedures to my patient in
I will explain all procedures to my patient in
order to allay anxiety.
order to allay anxiety.
47.
Psychological Support cont…
PsychologicalSupport cont…
I will involve the loved ones in his care in
I will involve the loved ones in his care in
order for him not to feel neglected.
order for him not to feel neglected.
I will involve him in planning his own care in
I will involve him in planning his own care in
order for him not to feel left out.
order for him not to feel left out.
48.
Hygiene
Hygiene
Patient isnursed in clean enviloment to prevent
Patient is nursed in clean enviloment to prevent
him from other respiratory conditions.
him from other respiratory conditions.
Sputum mug is provided to prevent
Sputum mug is provided to prevent
indiscriminate spitting.
indiscriminate spitting.
Since the patient is likely to sweat, i will
Since the patient is likely to sweat, i will
encourage him to take plunge baths in order to
encourage him to take plunge baths in order to
refresh his body.
refresh his body.
49.
Nutrition
Nutrition
I will provideoral fluids to prevent dehydration
I will provide oral fluids to prevent dehydration
due to excessive sweating.
due to excessive sweating.
I will serve small frequent meals to promote
I will serve small frequent meals to promote
appetite.
appetite.
Vegetables and fruits will be provided to raise
Vegetables and fruits will be provided to raise
the immunity and promote skin and mucous
the immunity and promote skin and mucous
membrane integrity.
membrane integrity.
50.
Elimination
Elimination
I willprovide a lot of fluids and roughage to
I will provide a lot of fluids and roughage to
prevent constipation.
prevent constipation.
I will provide fluids in moderation in order to
I will provide fluids in moderation in order to
maintain fluid balance in the body.
maintain fluid balance in the body.
Exercise
Exercise
I will encourage the patient to do deep
I will encourage the patient to do deep
breathing exercises in order to promote lung
breathing exercises in order to promote lung
expansion.
expansion.
51.
I.E.C
I.E.C
I willadvise the patient to be staying in a in a
I will advise the patient to be staying in a in a
clean environment which is dust free to prevent
clean environment which is dust free to prevent
triggering attacks.
triggering attacks.
I will advise the patient to identify allergens and
I will advise the patient to identify allergens and
avoid them in order to prevent frequent attacks.
avoid them in order to prevent frequent attacks.
52.
I.E.C
I.E.C
I willadvise my patient to continue with the
I will advise my patient to continue with the
prescribed treatment in order to achieve full
prescribed treatment in order to achieve full
recovery.
recovery.
I will emphasise the importance of seeking
I will emphasise the importance of seeking
early medical attention, keeping review dates
early medical attention, keeping review dates
and appointments.
and appointments.