Introduction
• The appendixis a wormlike extension of the cecum and, for this
reason, has been called the vermiform appendix.
• Its average length is 8-10 cm (ranging from 2-20 cm).
• Appendicitis is inflammation of the inner lining of the vermiform
appendix that spreads to its other parts.
• This illness is one of the most common surgical emergencies,
and it is one of the most common causes of abdominal pain.
3.
Introduction
• Statistics reportthat 1 of 5 cases of appendicitis is
misdiagnosed.
• Appendectomy is the only rational therapy for acute
appendicitis.
• It avoids clinical deterioration and may avoid chronic or
recurrent appendicitis.
• The incidence of acute appendicitis is around 7% of the
population in the United States and in European countries.
• In Asian and African countries, the incidence is probably
lower because of the dietary habits of the inhabitants of
these geographic areas.
4.
Introduction
• The higherincidence of appendicitis is believed to be related
to poor fiber intake in such countries.
• Rare cases of neonatal and prenatal appendicitis have been
reported.
• Appendicitis occurs more frequently in males than in
females, with a male-to-female ratio of 1.7:1.
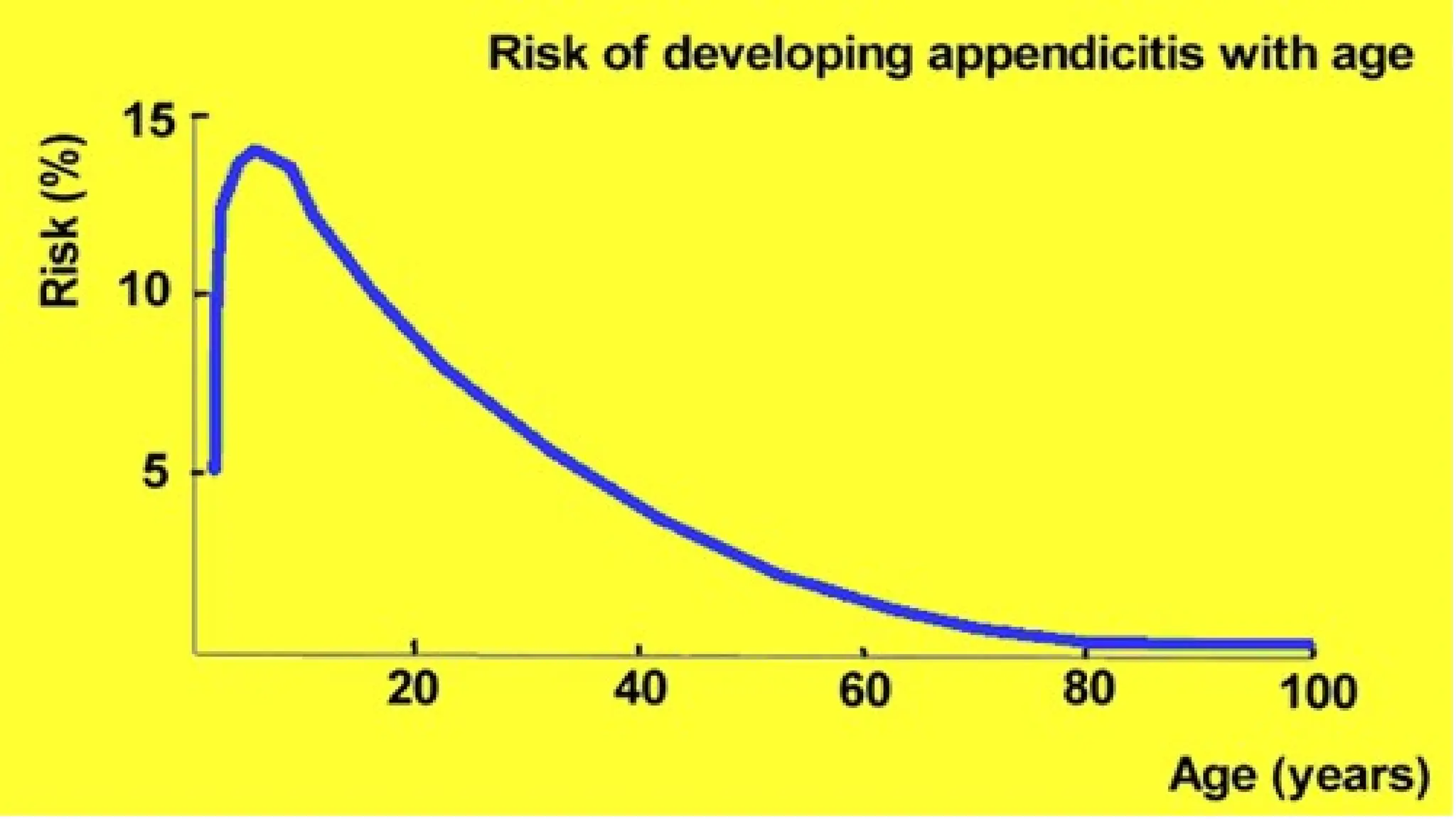
• Persons of any age may be affected, with highest incidence
occurring during the second and third decades of life.
5.
Essentials of background
•Acute Appendicitis is the most common acute abdomen.
• Appendicectomy is the most common emergency surgical
operation.
• Appendicitis can occur at any age but is most common
below 40 years, especially between the ages of 8 and 14.
• Acute appendicitis should be in the differential diagnosis of
all patients presenting to hospital with abdominal pain.
7.
Relevant Anatomy
• Theappendix is a wormlike extension of the cecum, and its
average length is 8-10 cm (ranging from 2-20 cm).
• This organ appears during the fifth month of gestation, and
its wall has an inner mucosal layer, 2 muscular layers, and a
serosa.
• Several lymphoid follicles are scattered in its mucosa.
• The number of follicles increases when individuals are aged
8-20 years.
• The inner muscular layer is circular, and the outer layer is
longitudinal and derives from the taenia coli.
8.
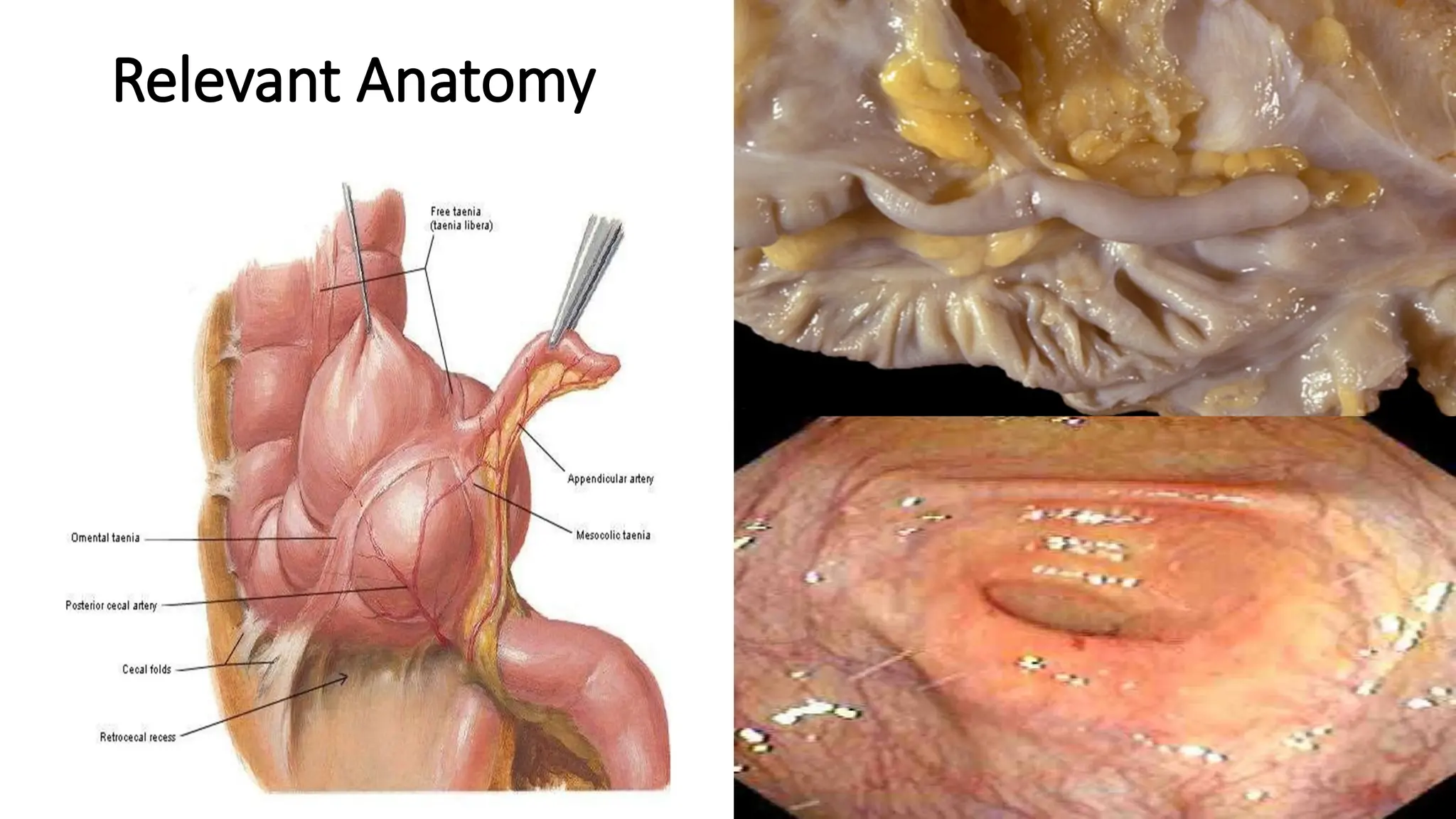
Relevant Anatomy
• Taeniacoli converge on the posteromedial area of the
cecum.
• This site is the appendiceal base.
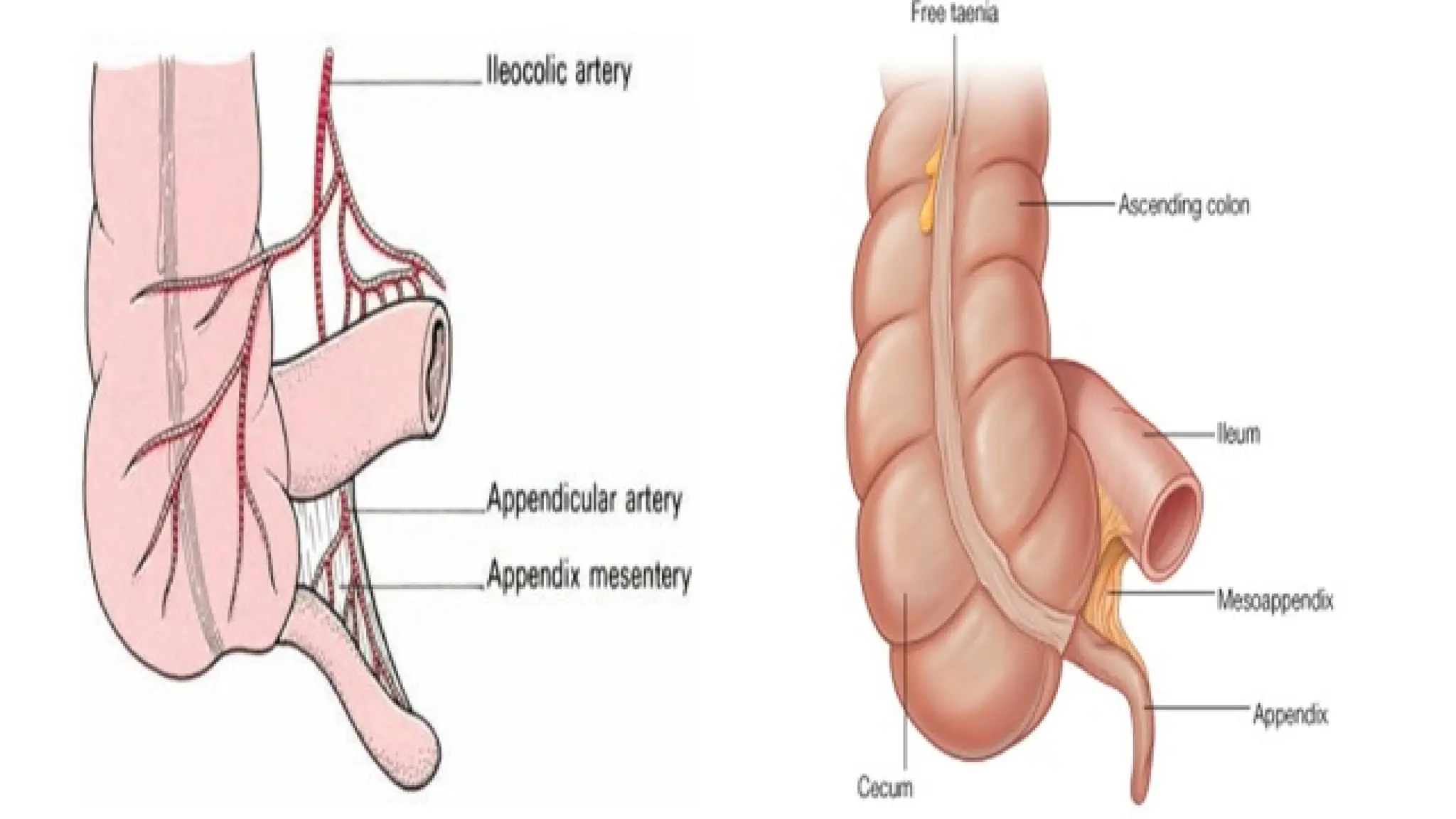
• The appendix runs into a serosal sheet of the peritoneum
called the mesoappendix.
• Within the mesoappendix courses the appendicular artery,
which is derived from the ileocolic artery.
• Sometimes, an accessory appendicular artery (deriving from
the posterior cecal artery) may be found.
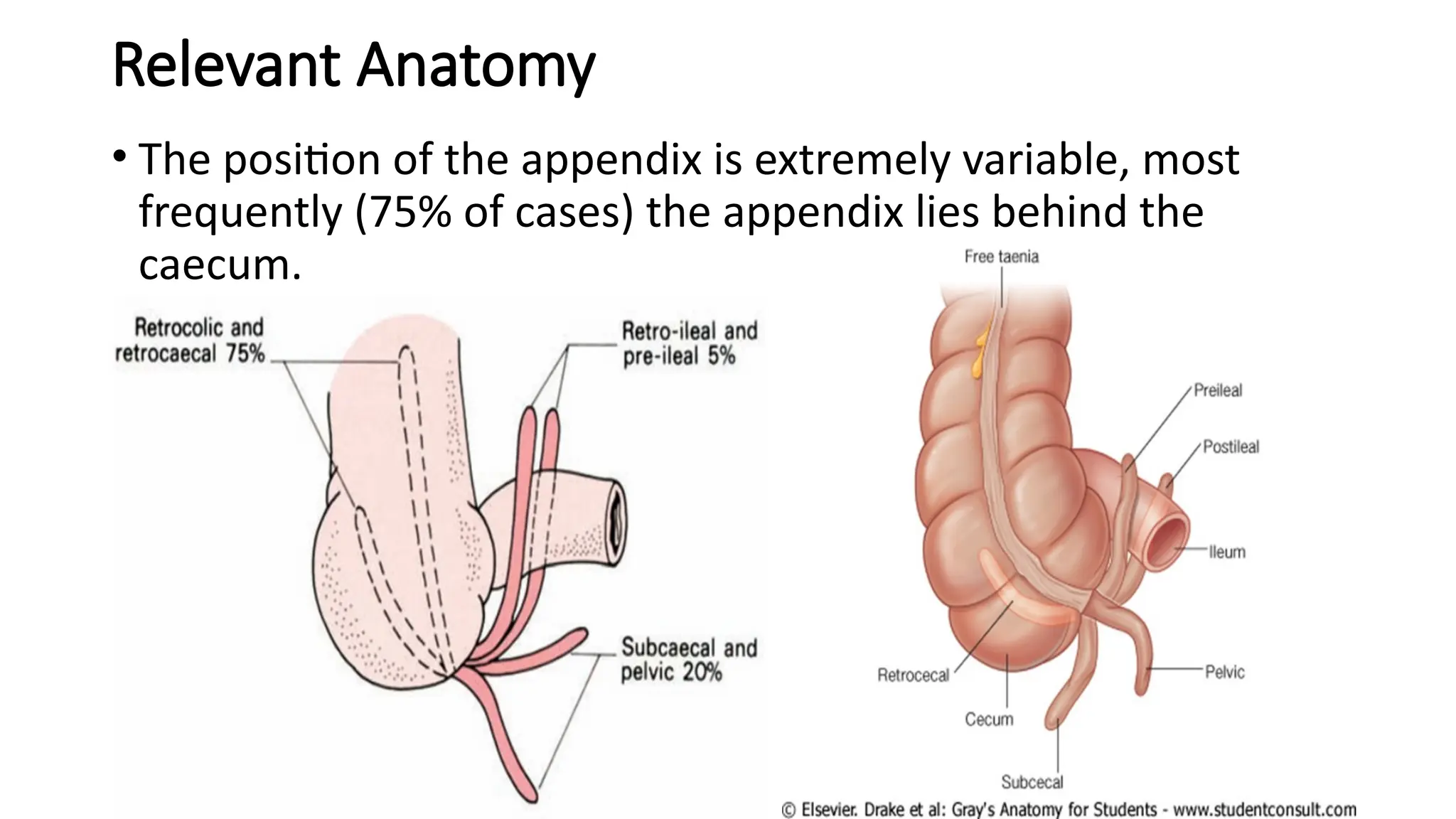
Relevant Anatomy
• Theposition of the appendix is extremely variable, most
frequently (75% of cases) the appendix lies behind the
caecum.
12.
Aetiology
• Appendicitis iscaused by obstruction of the appendiceal
lumen.
• The causes of the obstruction include
• Infections
• Fecal stasis and fecaliths
• Parasites
• Foreign bodies and neoplasms.
• Lymphoid hyperplasia may be related to Crohn disease,
mononucleosis, amebiasis, measles, and GI and respiratory
infections.
13.
Pathophysiology
• Appendicitis iscaused by obstruction of the appendiceal
lumen from a variety of causes.
• Obstruction is believed to cause an increase in pressure
within the lumen.
• Such an increase is related to continuous secretion of fluids
and mucus from the mucosa and the stagnation of this
material.
14.
Pathophysiology
• Intestinal bacteriawithin the appendix multiply, leading to
the recruitment of white cells and the formation of pus.
• This will lead to subsequent higher intraluminal pressure.
• If appendiceal obstruction persists, intraluminal pressure
rises ultimately above that of the appendiceal veins, leading
to venous outflow obstruction.
15.
Pathophysiology
• As aconsequence, appendiceal wall ischemia begins,
resulting in a loss of epithelial integrity and allowing bacterial
invasion of the appendiceal wall.
• Within a few hours, this localized condition may worsen
because of thrombosis of the appendicular artery and veins,
leading to perforation and gangrene of the appendix.
• As this process continues, a peri-appendicular abscess or
peritonitis may occur.
16.
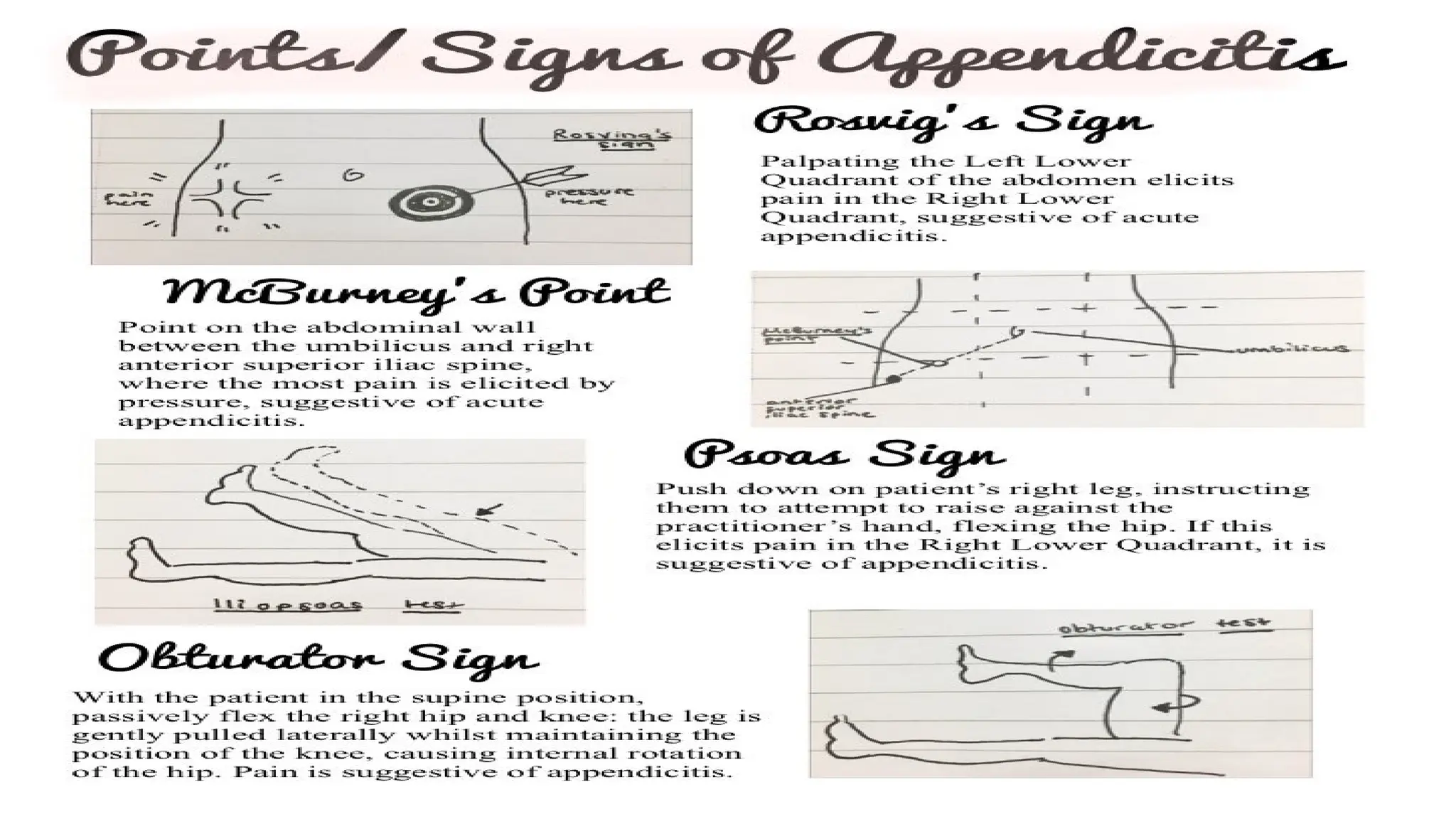
Clinical picture VsAnatomy
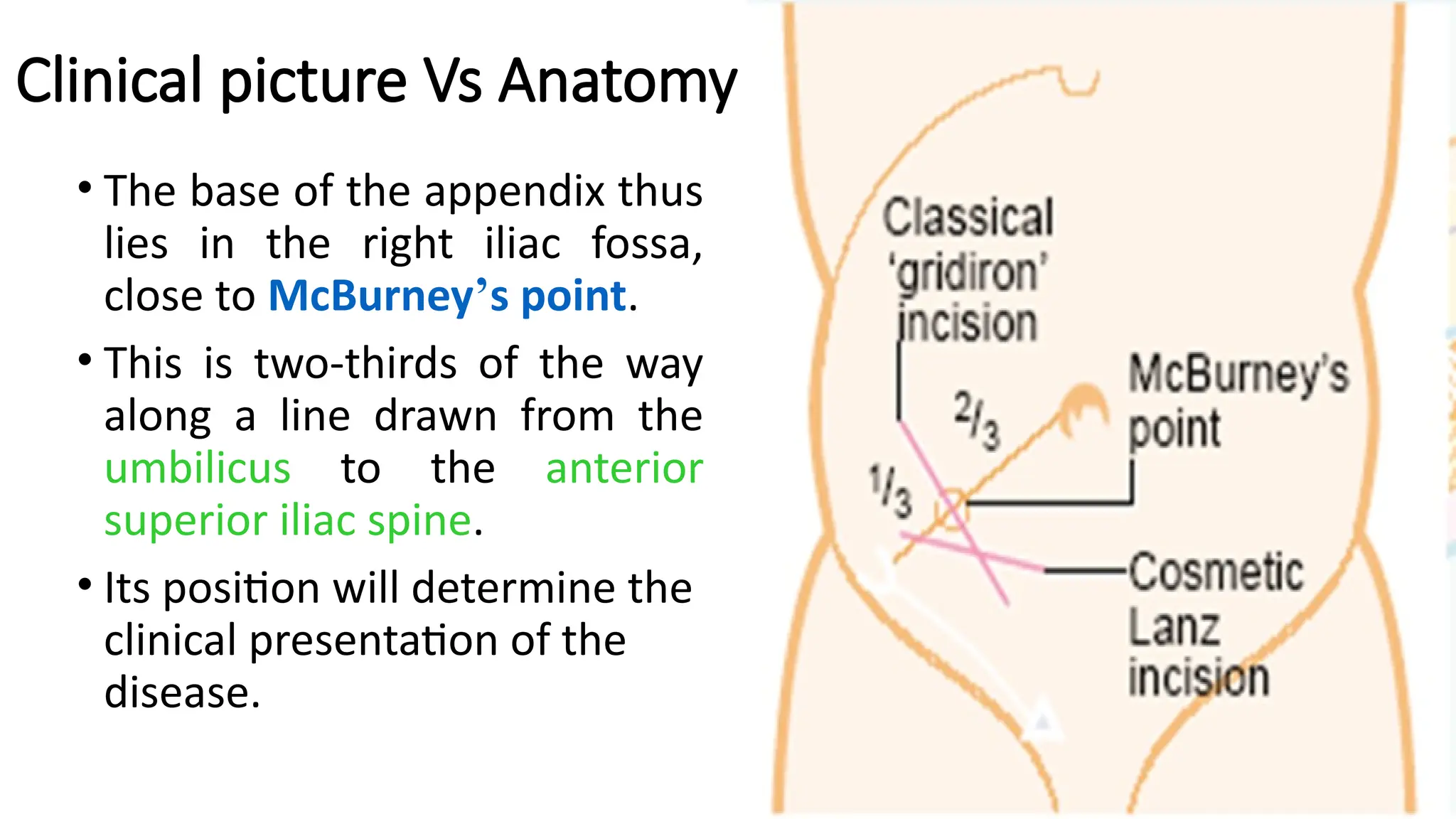
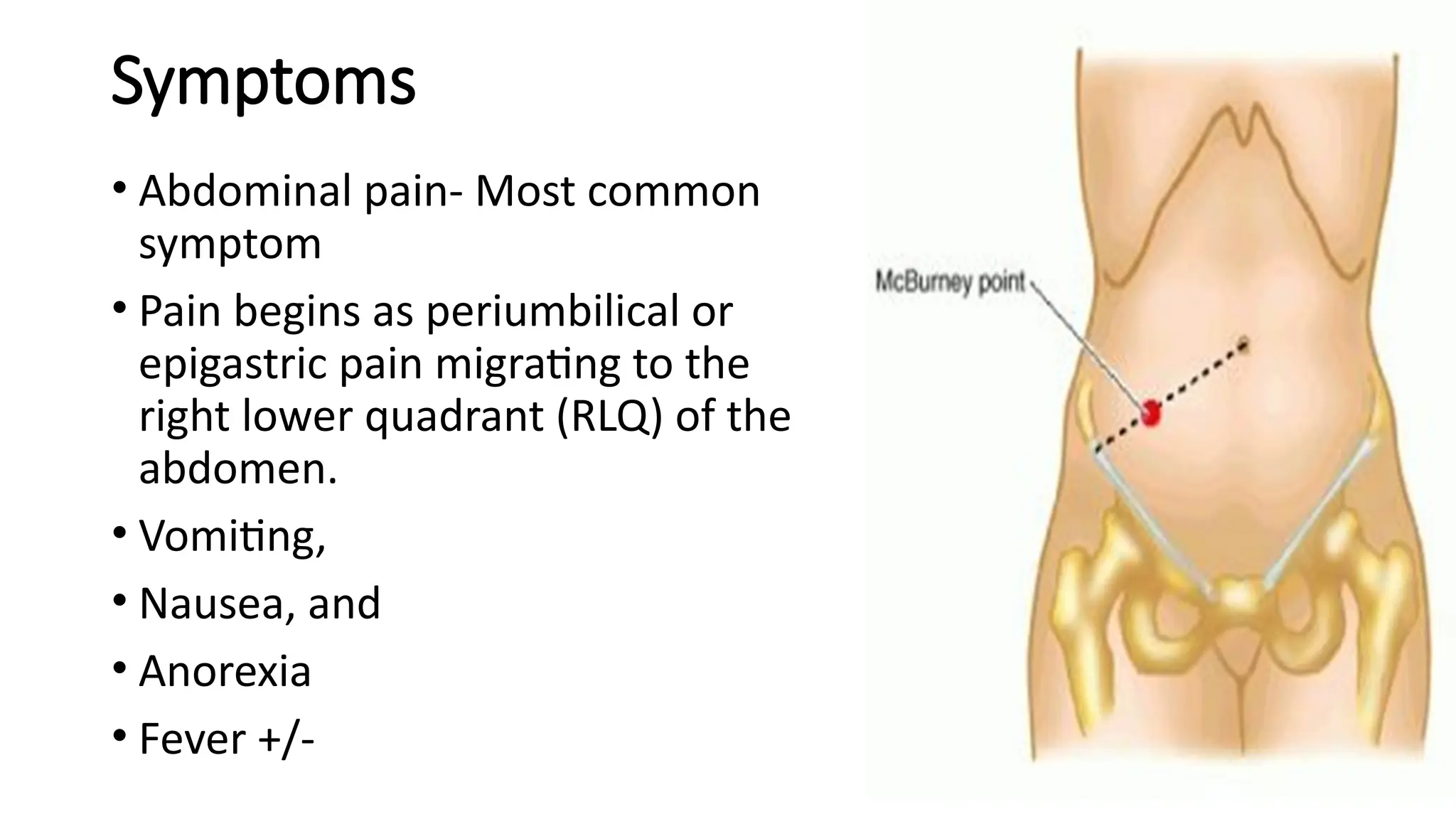
• The base of the appendix thus
lies in the right iliac fossa,
close to McBurney’s point.
• This is two-thirds of the way
along a line drawn from the
umbilicus to the anterior
superior iliac spine.
• Its position will determine the
clinical presentation of the
disease.
17.
Symptoms
• Abdominal pain-Most common
symptom
• Pain begins as periumbilical or
epigastric pain migrating to the
right lower quadrant (RLQ) of the
abdomen.
• Vomiting,
• Nausea, and
• Anorexia
• Fever +/-
18.
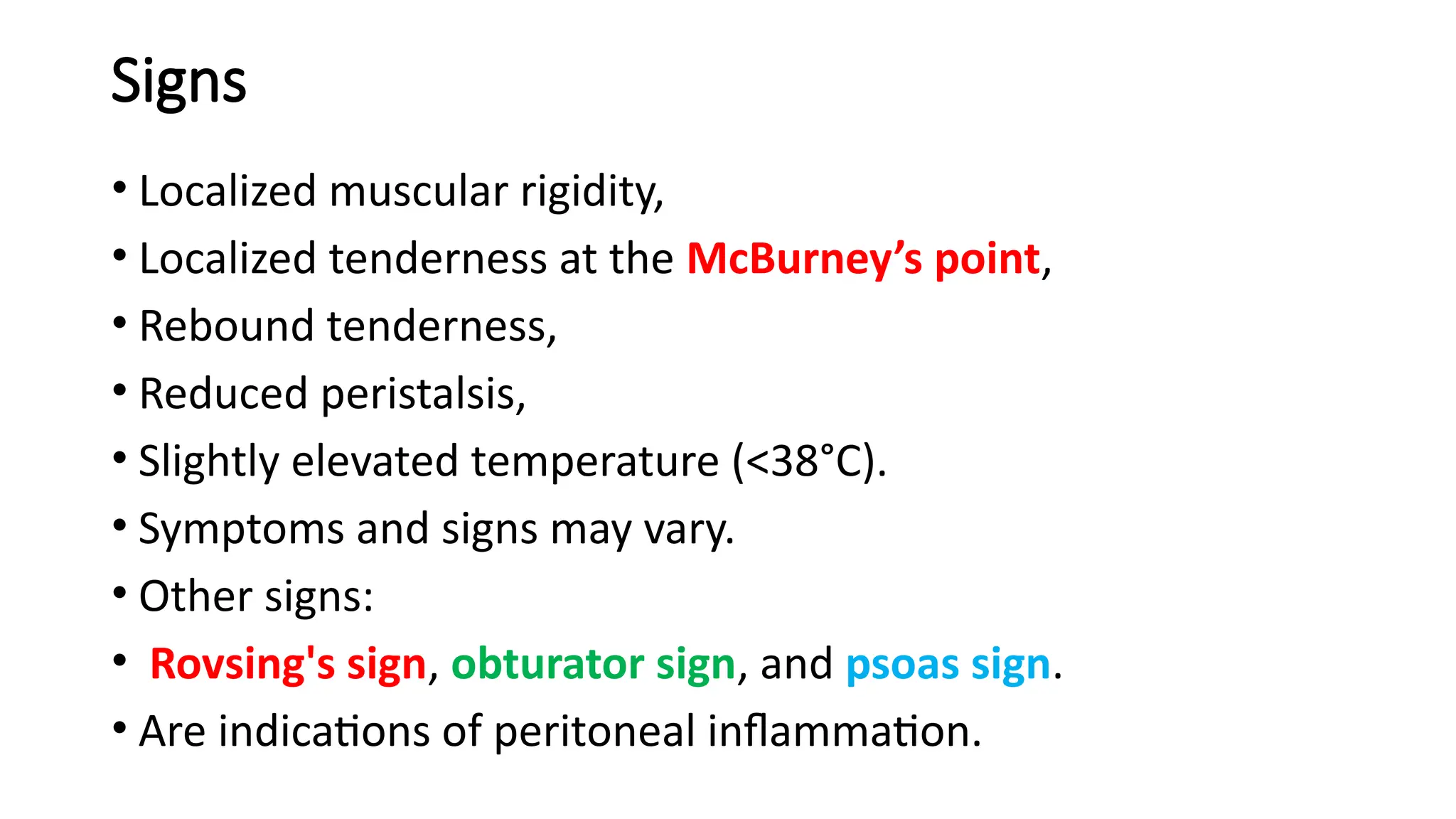
Signs
• Localized muscularrigidity,
• Localized tenderness at the McBurney’s point,
• Rebound tenderness,
• Reduced peristalsis,
• Slightly elevated temperature (<38°C).
• Symptoms and signs may vary.
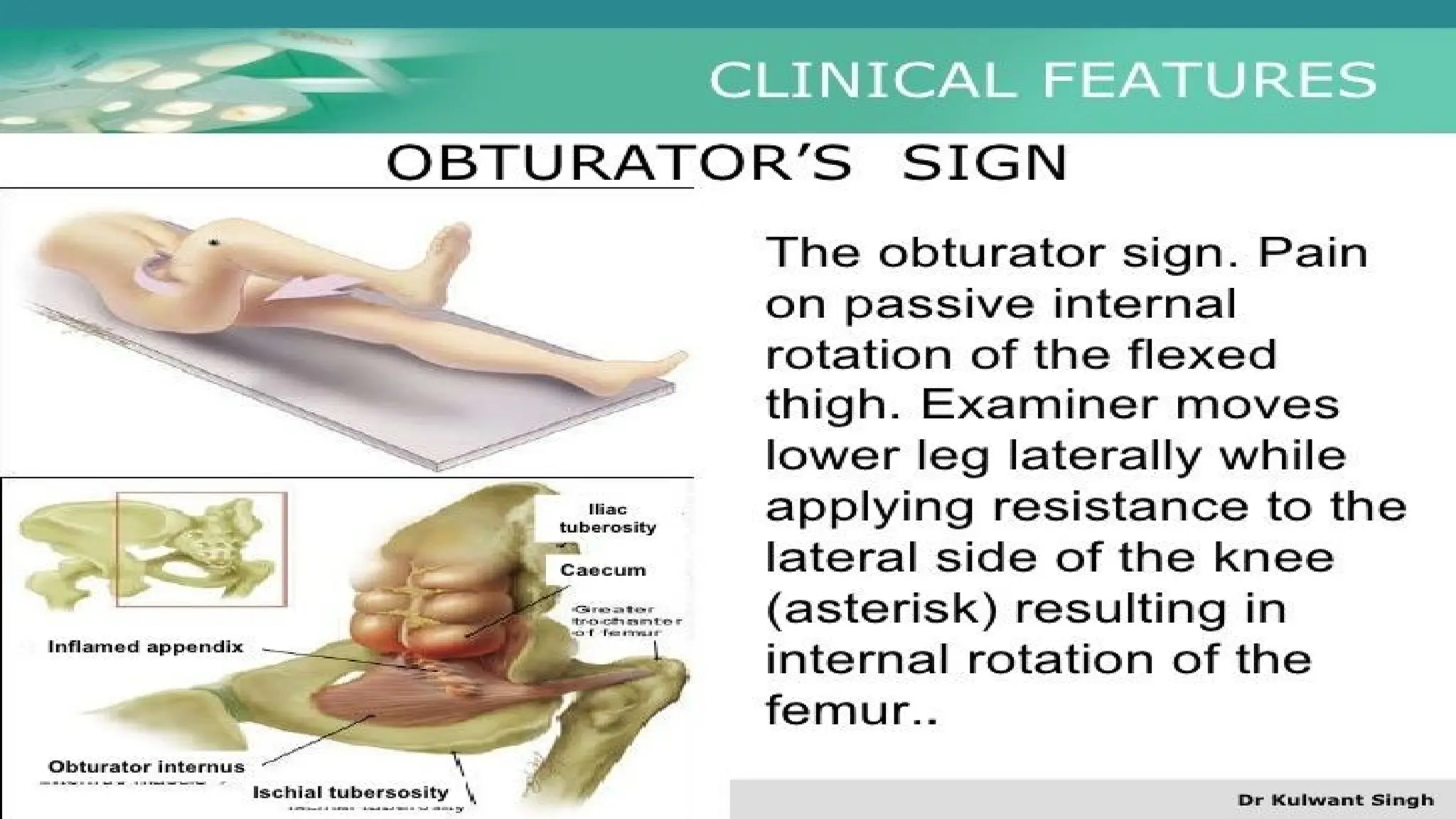
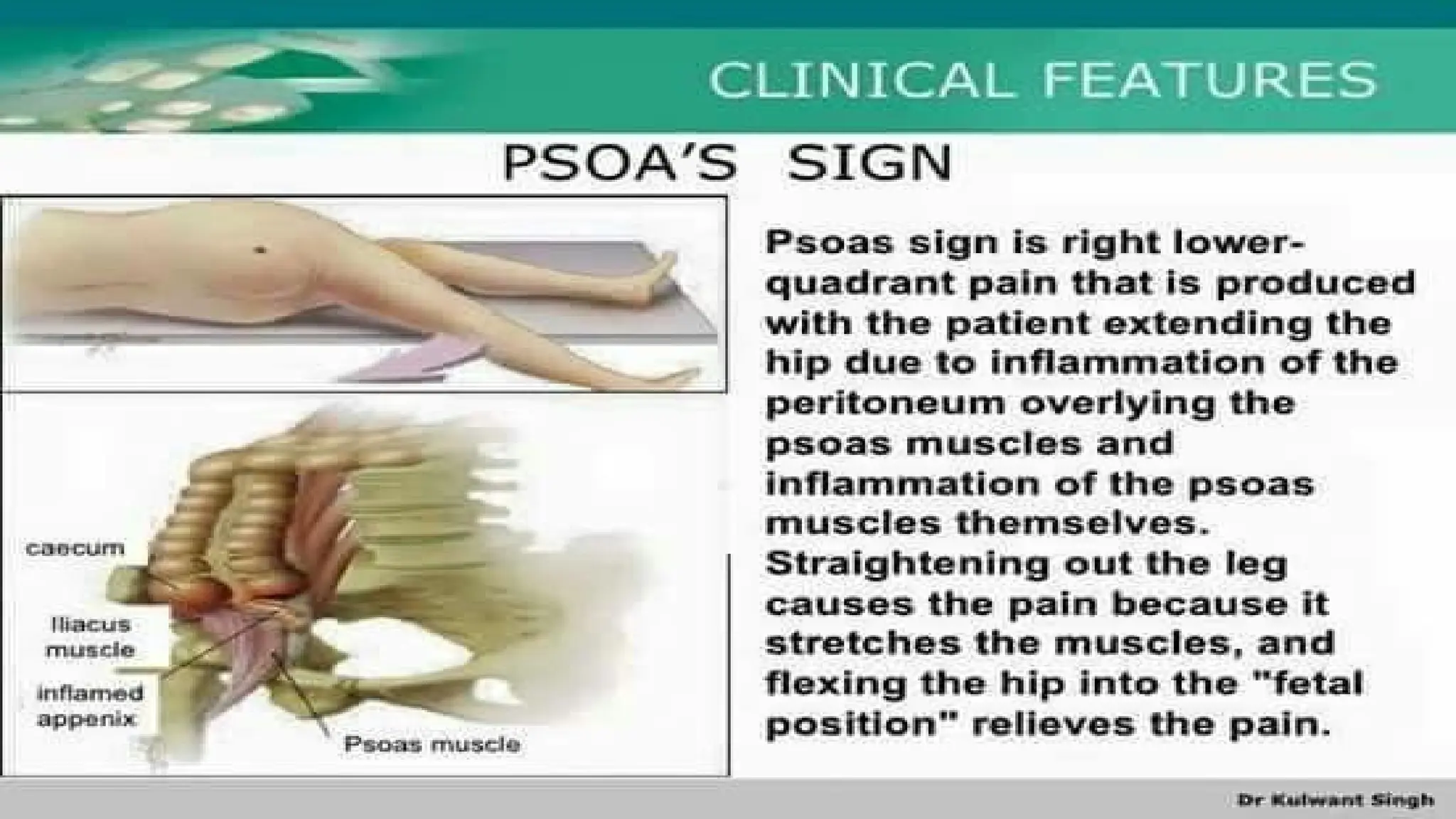
• Other signs:
• Rovsing's sign, obturator sign, and psoas sign.
• Are indications of peritoneal inflammation.
Investigations
• Appendicitis isessentially a clinical diagnosis
Laboratory tests
• Laboratory tests are not specific for appendicitis but may be
helpful to confirm diagnosis in patients with an atypical
presentation.
• Complete blood cell count
• Urinalysis
• C-reactive protein
• Liver and pancreatic function tests
• Gravindex test to R/O early ectopic pregnancy.
24.
Investigations
Imaging Studies:
• Abdomenplain film
• Barium enema
• Ultrasound
• Computed tomography scan
Diagnostic Procedures:
• Diagnostic laparoscopy may be useful in selected cases
25.
Complications-Perforation
• Perforation mayresult in localized or generalized peritonitis.
• Results in more sever pain, higher fever.
• Results in worse prognosis (more long-term complications
and higher mortality).
• Usually occur 12hrs after the onset, usually among children
and elderly people.
26.
Complications-Peritonitis
• Tenderness, rigidity,abdominal distention, adynamic ileus,
fever and toxicity.
• The severity of manifestations varies depending on if it is
localized or generalized peritonitis.
27.
Complications- Appendiceal abscess
•A right lower quadrant mass + typical course of appendicitis
• An ultrasound or CT scan is necessary for differentiation.
• Opinion differs about the treatment.
• Early operation under antibiotic cover is now performed
more frequently.
28.
Treatment
• Apendicectomy
• Antibioticsin support
• If perforation has occurred, then resuscitate before
operation
• Appendix mass
• When omentum and small bowel become adherent to the
inflamed appendix, give antibiotic, analgesia and iv fluids
and postpone operation and do interval Appendicectomy
after the mass has resolved
Introduction
• Peritonitis isan inflammation of the peritoneum, and can
be categorized as:
• Localized or diffuse
• Acute or Chronic
• According to the primary underlying pathology.
• In the clinical setting, the most useful categorization of
peritonitis is based on whether it is localized or diffuse.
Paths To PeritonealInfection
• Gastrointestinal perforation, e.g.
• Perforated ulcer
• Appendix
• Diverticulum
• Transmural translocation (no perforation), e.g.
• pancreatitis,
• ischaemic bowel,
• primary bacterial peritonitis
36.
Paths To PeritonealInfection
• Exogenous contamination, e.g.
• Drains,
• Open surgery,
• Trauma,
• Peritoneal dialysis
• Female genital tract infection, e.g.
• Pelvic inflammatory disease
• Haematogenous spread (rare), e.g.
• Septicaemia
37.
Localized peritonitis
• Thisis where a localized area of the peritoneum has become
inflamed.
• If the parietal peritoneum is involved, the patient complains
of pain in the area affected.
• Vital signs may be normal, but tachycardia and pyrexia are
common.
38.
Localized peritonitis
• Thecharacteristic signs are:
• Involuntary guarding- reflex abdominal wall contraction to
reduce further peritoneal irritation.
• Rebound tenderness- worsening of pain on lifting the
examining hand of the abdominal wall).
• Collectively these signs and symptoms are termed
peritonism and the patient is described as peritonitic
39.
Diffuse (generalized) peritonitis
•This signifies the occurrence of a life-threatening condition.
• It normally arises as a result of pressure-related perforation
of a viscus.
• Maybe acute or gradual onset severe abdominal pain.
• The pain may be localized at first and then become diffuse.
• The patient is gravely ill looking
40.
Diffuse (generalized) peritonitis
•There is board-like’ rigidity on abdominal palpation.
• A generalized ileus occurs and the abdomen may become
distended.
• Vital signs are usually deranged.
• In advanced cases the patient is hypotensive, tachycardic and
pyrexial.
41.
Diffuse (generalized) peritonitis
•At first the patient may seem confused, drowsy and
disoriented.
• If the underlying pathology is not corrected the patient will
lose consciousness.
• Signs may be limited in obese patients or in patients on
immunosuppressive medications.
42.
Clinical features ofperitonitis
• Abdominal pain, worse on movement, coughing and deep
respiration
• Constitutional upset: anorexia, malaise, fever, lassitude
• Gastrointestinal upset: nausea +/– vomiting
• Raised pulse rate, +/- Pyrexia
• Tenderness +/– guarding/rigidity/rebound of abdominal wall
• Pain/tenderness on rectal/vaginal examination (pelvic
peritonitis)
• Absent or reduced bowel sounds
• Septic shock
43.
Management of peritonitis
Generalcare of patient
• Correction of fluid and electrolyte imbalance
• Insertion of nasogastric drainage tube and urinary catheter
• Broad-spectrum antibiotic therapy
• Analgesia
• Vital system support
Surgical treatment of cause when appropriate
• ‘Source control’ by removal or exclusion of the cause
• Peritoneal lavage +/– drainage