Download to read offline

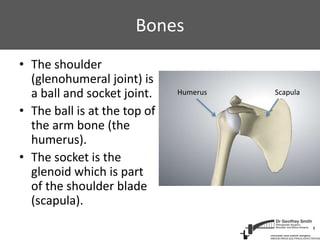

This document provides information about shoulder arthroscopic stabilization surgery. It describes how arthroscopy uses small incisions and a camera to view the inside of the shoulder joint. During surgery, torn ligaments and labrum from shoulder dislocations are reattached to the shoulder bone using suture anchors to stabilize the joint and prevent further dislocations. The recovery process involves wearing a sling for 6 weeks followed by strengthening exercises, with a full return to activities in 4-6 months.
















































































