Downloaded 23 times
















































































































































![SENSING FUNCTION:
Cardiac pacemaker have the
ability to see intrinsic cardiac Activity
when it occurs.
CAPTURE FUNCTION:
The ability to generate a response
from the heart [contraction] after
electrical stimulation is referred as
capture.](https://image.slidesharecdn.com/dysrhythmia-240124221341-c62adf2f/75/Dysrhythmia-pptx-146-2048.jpg)












![Patient education
• Check pulse daily.
• Avoid weight lifting.[>20 lb]
• Avoid shower.
• Avoid lifting hand over shoulder level.
• Wear loose-fitting clothing.
• Avoid trauma to the area.
• Come for regular check up.](https://image.slidesharecdn.com/dysrhythmia-240124221341-c62adf2f/75/Dysrhythmia-pptx-159-2048.jpg)



























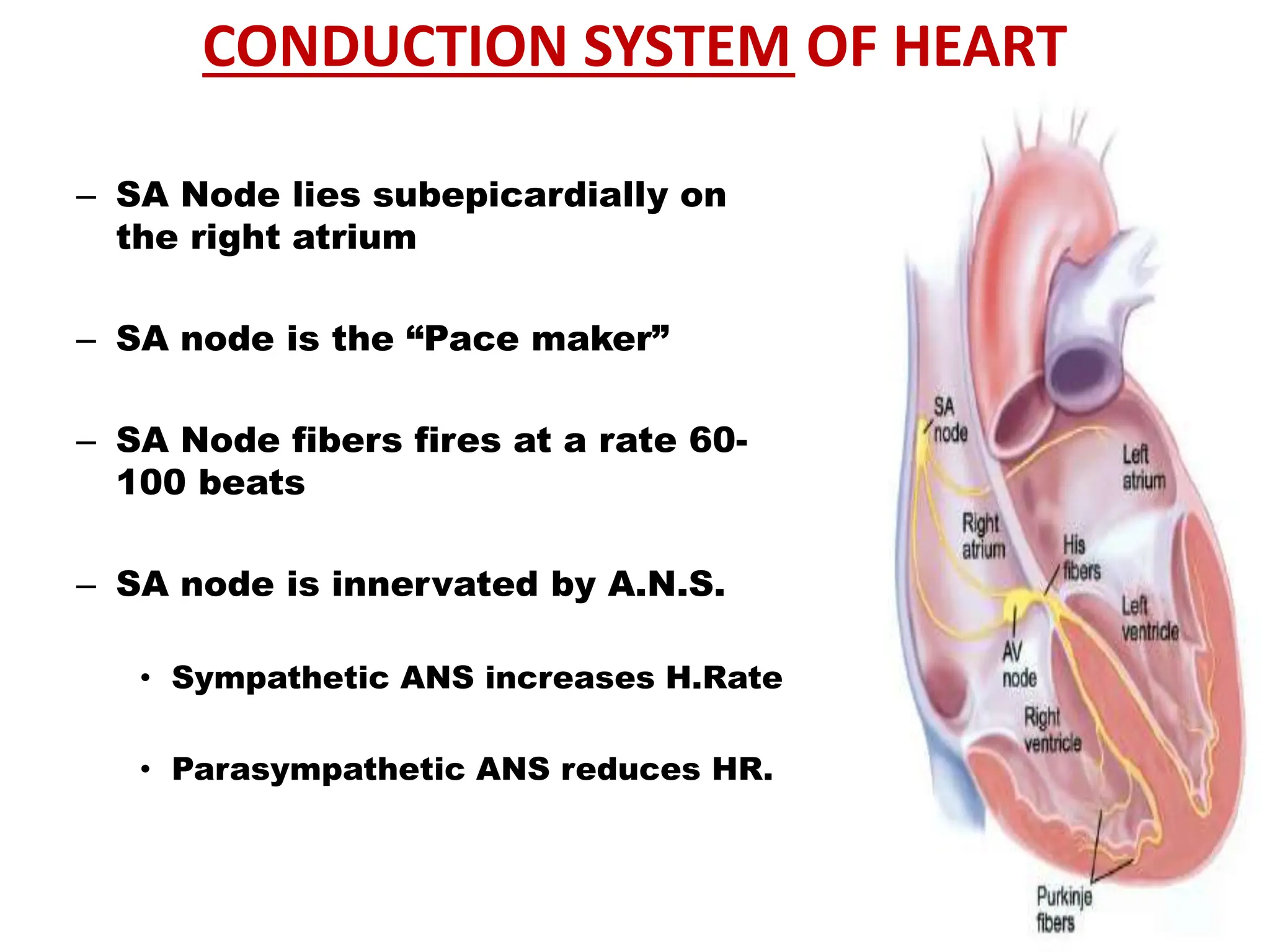
The document discusses the conduction system of the heart and various cardiac arrhythmias or dysrhythmias. It describes the normal conduction pathway beginning with the sinoatrial node and discusses how arrhythmias can result from disturbances to automaticity, conduction or reentry of impulses. Several specific types of arrhythmias are described including sinus node dysrhythmias, atrial arrhythmias, AV junctional dysrhythmias and ventricular dysrhythmias. Causes, characteristics, clinical manifestations and treatment approaches are provided for select arrhythmias such as sinus tachycardia, sinus bradycardia and sick sinus syndrome.










































































