Recommended

Recommended
More Related Content
Recently uploaded
Recently uploaded (20)
Featured
Featured (20)
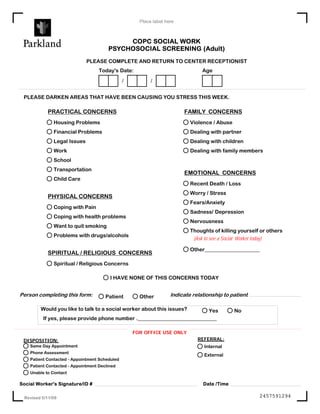
Psychosocial Screening Tool
- 1. Place label here COPC SOCIAL WORK PSYCHOSOCIAL SCREENING (Adult) PLEASE COMPLETE AND RETURN TO CENTER RECEPTIONIST Today's Date: Age / / PLEASE DARKEN AREAS THAT HAVE BEEN CAUSING YOU STRESS THIS WEEK. PRACTICAL CONCERNS FAMILY CONCERNS Housing Problems Violence / Abuse Financial Problems Dealing with partner Legal Issues Dealing with children Work Dealing with family members School Transportation EMOTIONAL CONCERNS Child Care Recent Death / Loss Worry / Stress PHYSICAL CONCERNS Fears/Anxiety Coping with Pain Sadness/ Depression Coping with health problems Nervousness Want to quit smoking Thoughts of killing yourself or others Problems with drugs/alcohols (Ask to see a Social Worker today) Other_____________________ SPIRITUAL / RELIGIOUS CONCERNS Spiritual / Religious Concerns I HAVE NONE OF THIS CONCERNS TODAY Person completing this form: Patient Other Indicate relationship to patient Would you like to talk to a social worker about this issues? Yes No If yes, please provide phone number .______________________________ FOR OFFICE USE ONLY DISPOSITION: REFERRAL: Same Day Appointment Internal Phone Assessment External Patient Contacted - Appointment Scheduled Patient Contacted - Appointment Declined Unable to Contact Social Worker's Signature/ID # Date /Time Revised 5/11/09 2457591294