Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (17)
Similar to Aprepitantposter_final
Similar to Aprepitantposter_final (20)
Aprepitantposter_final
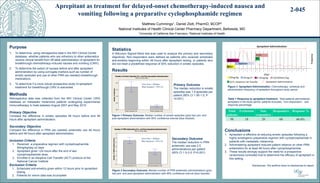
- 1. Matthew Cummings1, Daniel Zlott, PharmD, BCOP2 National Institutes of Health Clinical Center Pharmacy Department, Bethesda, MD 1University of California San Francisco; 2National Institutes of Health Purpose 1. To determine, using retrospective data in the NIH Clinical Center database, whether patients who are refractory to other antiemetics receive clinical benefit from off-label administration of aprepitant for breakthrough chemotherapy-induced nausea and vomiting (CINV). 2. To determine the extent of nausea before and after aprepitant administration by using surrogate markers such as number of emetic episodes and use of other PRN (as needed) breakthrough medications. 3. To determine if a more robust prospective study of aprepitant treatment for breakthrough CINV is warranted. Methods Retrospective data was collected from the NIH Clinical Center CRIS database on metastatic melanoma patients undergoing experimental immunotherapy in trials between August 2007 and May 2015. Primary Objective Compare the difference in emetic episodes 48 hours before and 48 hours after aprepitant administration. Secondary Objective Compare the difference in PRN (as needed) antiemetic use 48 hours before and 48 hours after aprepitant administration. Inclusion Criteria 1. Received a preparative regimen with cyclophosphamide 60mg/kg/day x2 days 2. Aprepitant given >24 hours after the end of last cyclophosphamide dose 3. Enrolled in an Adoptive Cell Transfer (ACT) protocol at the National Cancer Institute Exclusion Criteria 1. Scheduled anti-emetics given within 12 hours prior to aprepitant dosing 2. Patients for whom data was incomplete Conclusions 1. Aprepitant is effective at reducing emetic episodes following a highly emetogenic preparative regimen with cyclophosphamide in patients with metastatic melanoma. 2. Administering aprepitant reduced patient reliance on other PRN antiemetics for at least 48 hours after cylcophosphamide. 3. These results strongly support the need for a prospective randomized controlled trial to determine the efficacy of aprepitant in this setting. Disclosures: The authors have no disclosures to report. Aprepitant as treatment for delayed-onset chemotherapy-induced nausea and vomiting following a preparative cyclophosphamide regimen Figure 3 Aprepitant Administration. Chemotherapy schedule and administration frequency of aprepitant throughout study period. Statistics A Wilcoxon Signed-Rank test was used to analyze the primary and secondary objectives. Non-responders were defined as patients who received scheduled anti-emetics beginning within 48 hours after aprepitant dosing, or patients who did not meet a predefined response of 50% reduction in emetic episodes. Table 1 Response to aprepitant treatment. Total patients administered aprepitant in the study period, patients excluded, “non-responders” , and response percentage. Total patients Exclusions Non- responders Responders Response % 98 18 20 60 66.6% 2-045 Emetic Episodes PostEmetic Episodes Pre 2.0 1.5 1.0 0.5 0.0 NumberofEpisodes Number of Emetic Episodes Pre- and Post-Aprepitant Administration 95% CI for the Mean Grey bars = Median Blue brackets = 95% CI PRN Administrations PostPRN Administrations Pre 7 6 5 4 3 2 1 0 NumberofPRNAdministrations Number of PRN Antiemetics Pre- and Post-Aprepitant Administration 95% CI for the Mean Grey bars = Median Blue brackets = 95% CI Results Secondary Outcome The median reduction in PRN antiemetic use was 2.5 administrations per patient (95% CI 1.5-3.0; P<0.001). Primary Outcome The median reduction in emetic episodes was 1.5 episodes per patient (95% CI 1.00-1.5; P <0.001). Figure 1 Primary Outcome. Median number of emetic episodes (grey bar) pre- and post-aprepitant administration with 95% confidence interval (blue bracket). Figure 2 Secondary Outcome. Median number of PRN antiemetic administrations (grey bar) pre- and post aprepitant administration with 95% confidence interval (blue bracket).