
Recommended
More Related Content
Similar to Appendicitis ,pathophysiology and its management
Similar to Appendicitis ,pathophysiology and its management (20)
Recently uploaded
Recently uploaded (20)
Appendicitis ,pathophysiology and its management
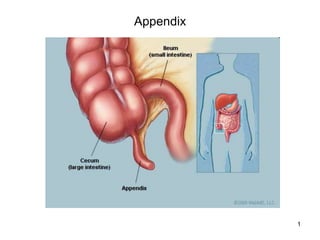
- 1. 1 Appendix
- 2. 2 Appendicitis • The appendix is a small, finger-like tube about 10 cm (4 in) long that is attached to the cecum just below the ileocecal valve. The appendix fills with food and empties regularly into the cecum. Because it empties inefficiently and its lumen is small, the appendix is prone to obstruction and is particularly vulnerable to infection (ie, appendicitis). In the adult, the average length of the appendix is 6 to 9 cm; however, it can vary in length from <1 to >30 cm. The outer diameter varies between 3 and 8 mm, whereas the luminal diameter varies between 1 and 3 mm. The appendix receives its arterial supply from the appendicular branch of the ileocolic artery. This artery originates posterior to the terminal ileum, entering the mesoappendix close to the base of the appendix. The lymphatic drainage of the appendix flows into lymph nodes that lie along the ileocolic artery. Innervation of the appendix is derived from sympathetic elements contributed by the superior mesenteric plexus (T10-L1) and afferents from the parasympathetic elements via the vagus nerves.
- 3. 3 Pathophysiology • The appendix becomes inflamed and edematous as a result of either becoming kinked or occluded by a fecalith (ie, hardened mass of stool), tumor, or foreign body. The inflammatory process increases intraluminal pressure, initiating a progressively severe, generalized or upper abdominal pain that becomes localized in the right lower quadrant of the abdomen within a few hours.
- 4. 4 Clinical Manifestations • Epigastric or periumbilical pain progresses to the right lower quadrant. • Low-grade fever, nausea and sometimes vomiting. Loss of appetite. • Local tenderness is elicited at McBurney’s point when pressure is applied. • Rebound tenderness (ie, production or intensification of pain when pressure is released) may be present. • Rovsing’s sign may be elicited by palpating the left lower quadrant; this causes pain to be felt in the right lower quadrant. • If the appendix has ruptured, the pain becomes more diffuse; abdominal distention develops, and the patient’s condition worsens.
- 5. 5 Location of McBurney's point (1), located two thirds the distance from the umbilicus (2) to the anterior superior iliac spine (3).
- 6. 6 Assessment and Diagnostic Findings • Health history and physical exam. • Complete blood cell count demonstrates an elevated white blood cell count (> 10,000 cells/mm3). The neutrophil count may exceed 75%. • Abdominal x-ray films, ultrasound studies, and CT scans may reveal a right lower quadrant density or localized distention of the bowel.
- 7. 7
- 8. 8 Medical Management • Surgical intervention (appendectomy), as soon as possible after diagnosis to decrease the risk of perforation. • Before surgery, correction or prevention of fluid and electrolyte imbalance and dehydration could be through antibiotics and intravenous fluids. • Analgesics can be administered after the diagnosis is made.
- 9. 9 An appendectomy in progress
- 10. 10 Management • Prepare the patient for surgery, which includes an intravenous infusion to replace fluid loss and promote adequate renal function and antibiotic therapy to prevent infection. • Post-operatively, Place the patient in a semi-Fowler position to reduce the tension on the incision and, thus, reduce pain. • Administer pain killers (usually morphine sulfate), as prescribed. • Start oral fluids when tolerated and intravenous fluids as indicated. Food is provided as desired and tolerated on the day of surgery.
- 11. 11 Management (Continued…..) • Instruct the patient to make an appointment to have the surgeon remove the sutures between the fifth and seventh days after surgery. • Teach incision care (dressing) and activity guidelines; normal activity can usually be resumed within 2 to 4 weeks.