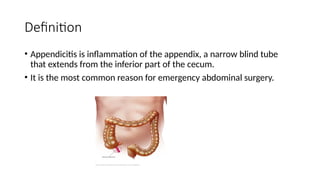
Appendicitis is the inflammation of the appendix, often resulting from obstruction, leading to severe abdominal pain and potential rupture. Key symptoms include right lower quadrant pain, fever, and loss of appetite, and diagnosis is typically confirmed via imaging and elevated white blood cell counts. The standard treatment is an immediate appendectomy, and nursing management focuses on pain relief and preventing complications.





































![Oxygenation 1st yr corrected 02 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/oxygenation1styrcorrected02autosaved-250107063557-199b5b45-thumbnail.jpg?width=640&height=640&fit=bounds)






























