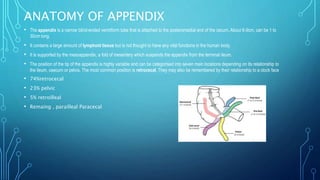
Appendicitis is inflammation of the vermiform appendix. It is most common in young adults and is caused by obstruction of the appendix lumen, usually by a fecalith. Without treatment, bacterial overgrowth and ischemia can lead to appendiceal necrosis and perforation. Acute appendicitis presents with abdominal pain localized to the right lower quadrant. Delayed treatment increases risk of complications like perforation and abscess. Surgical removal of the appendix (appendectomy) is the standard treatment for acute appendicitis.