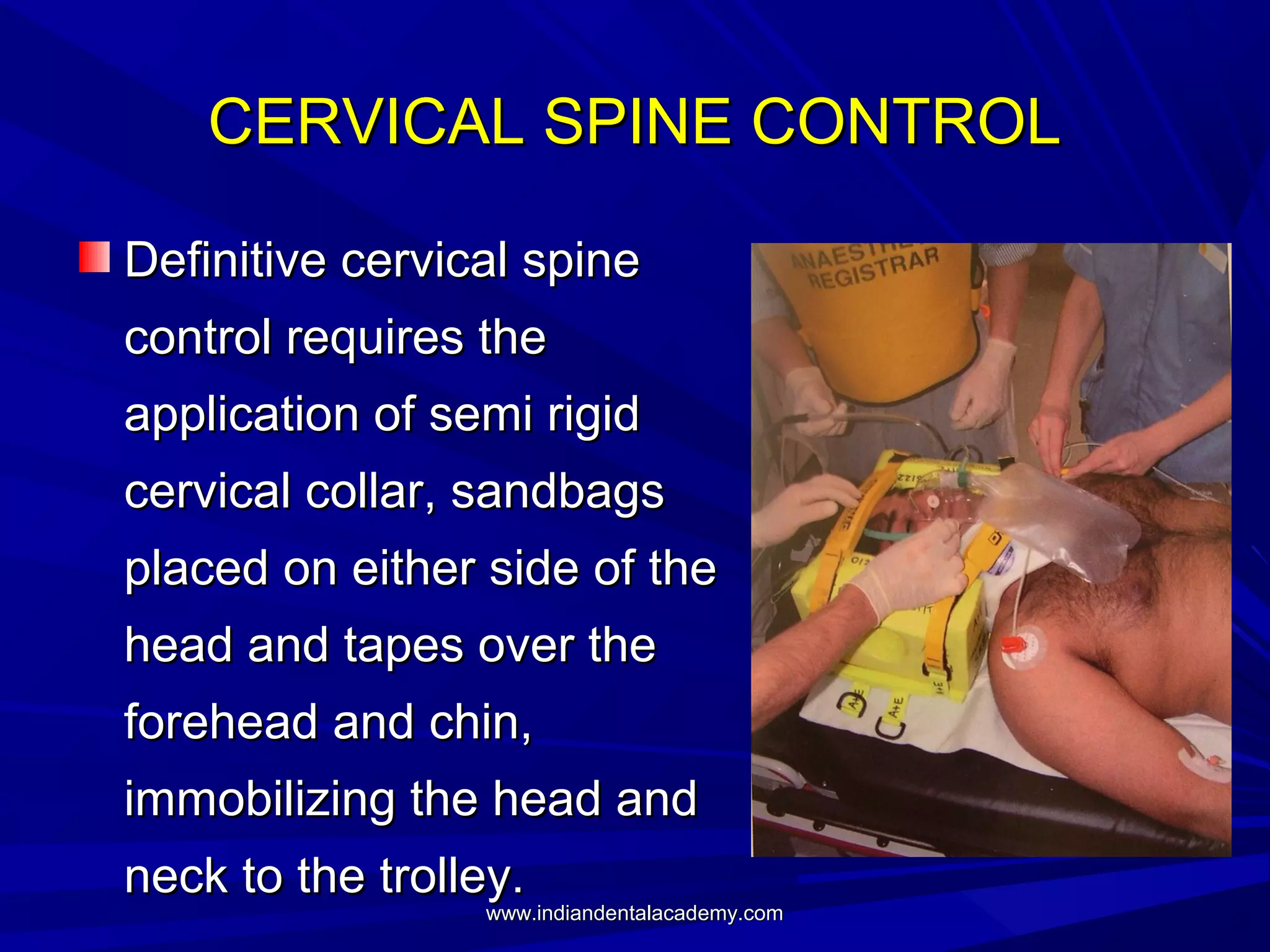
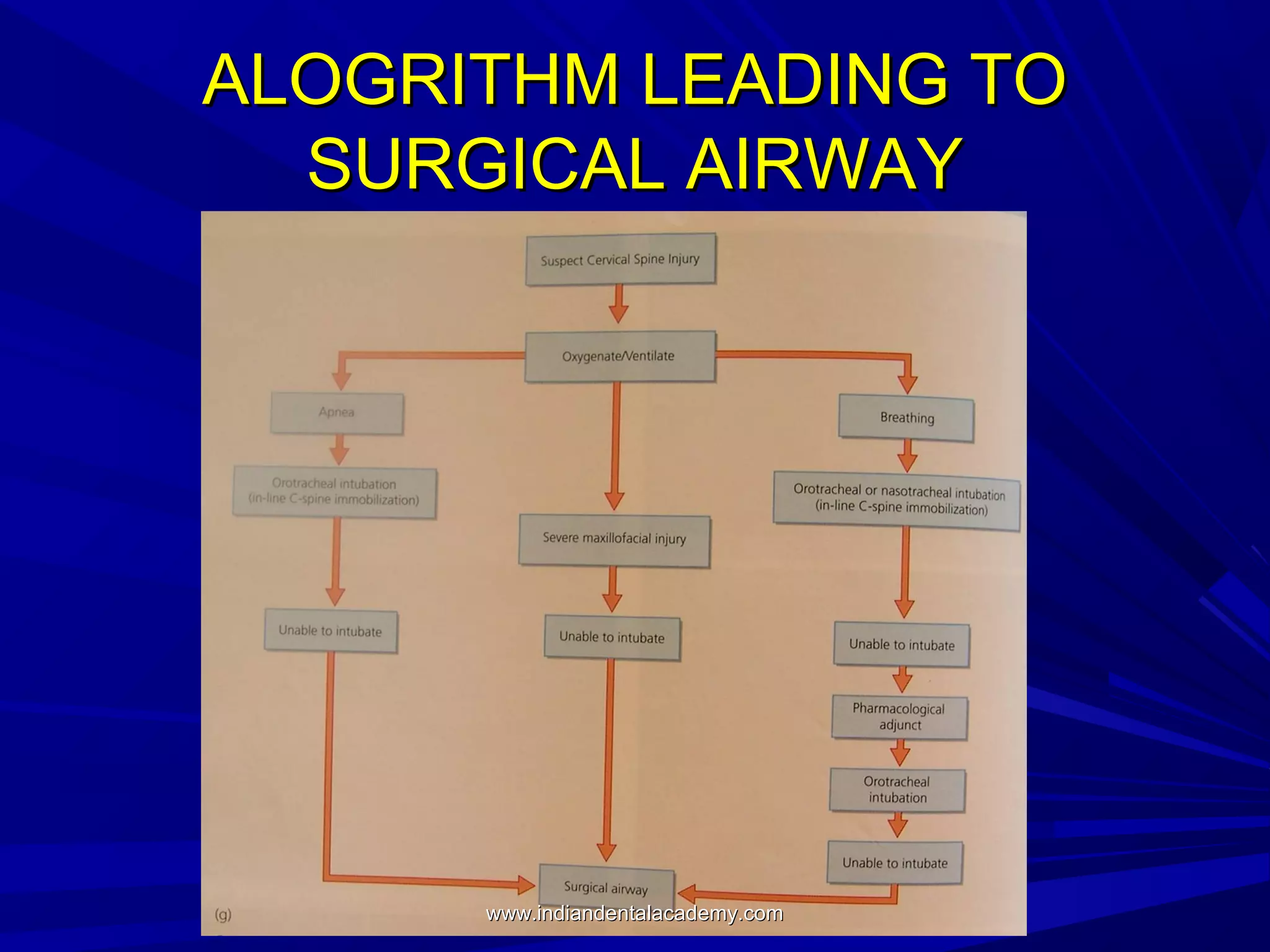







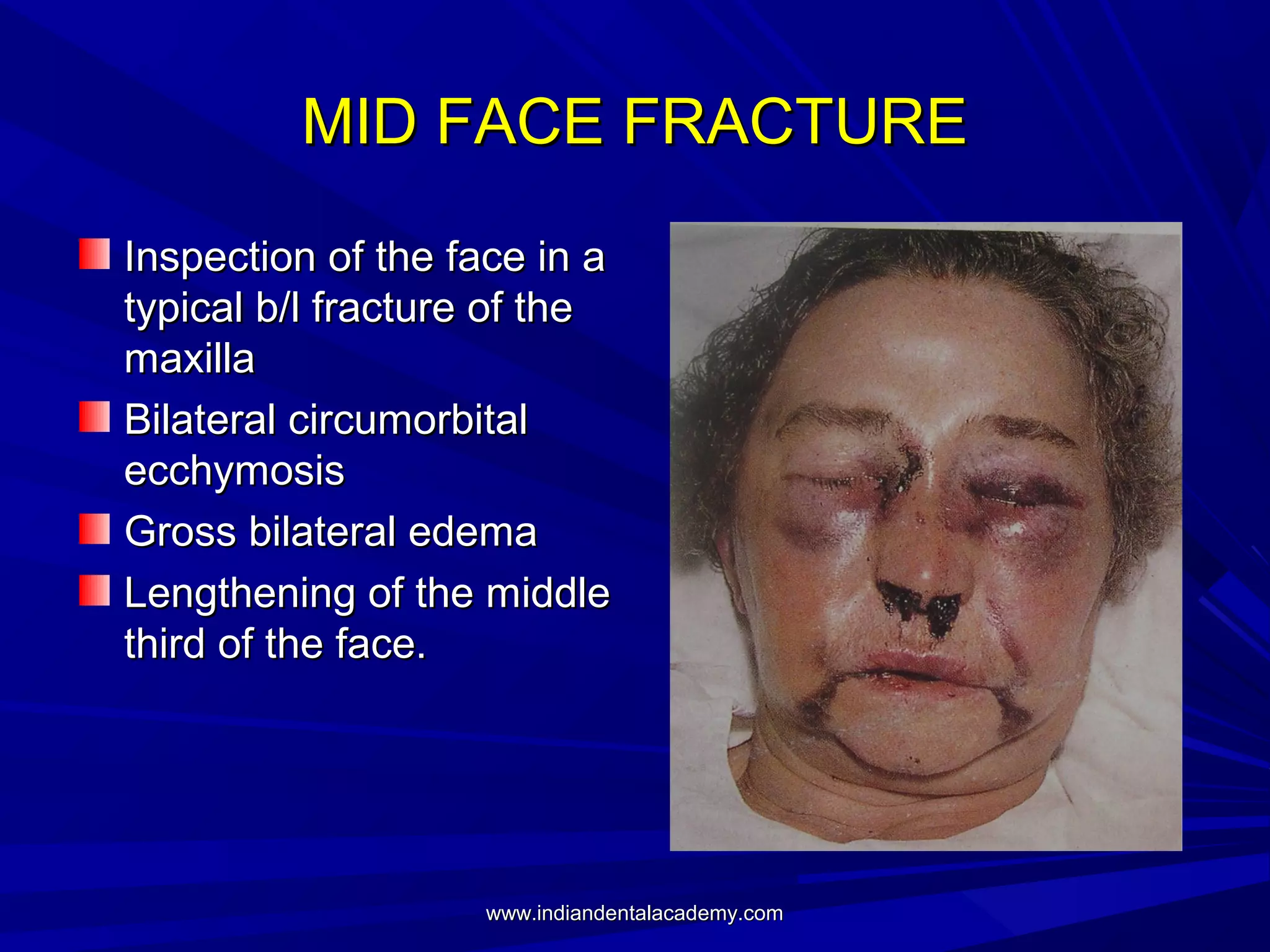

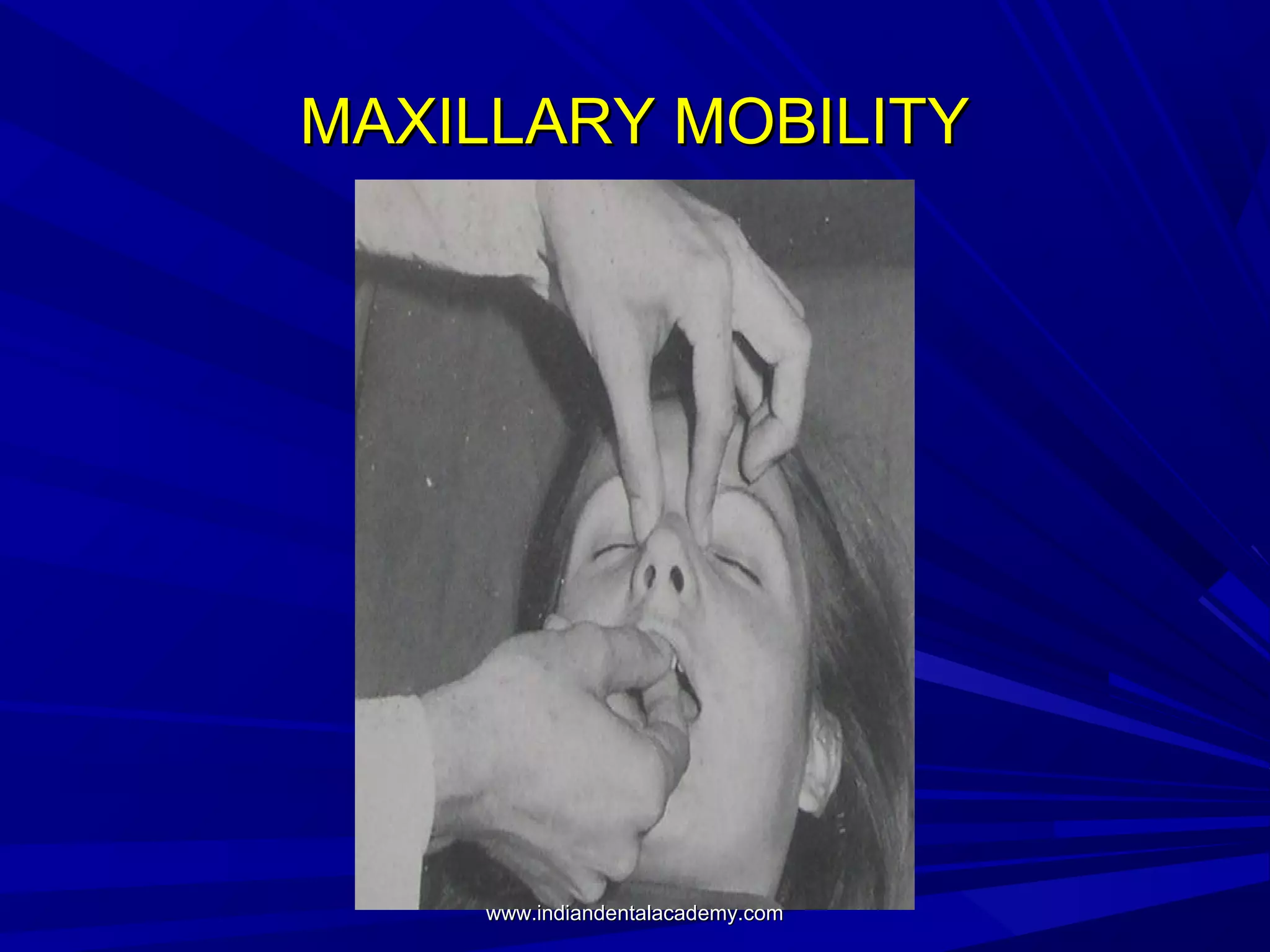
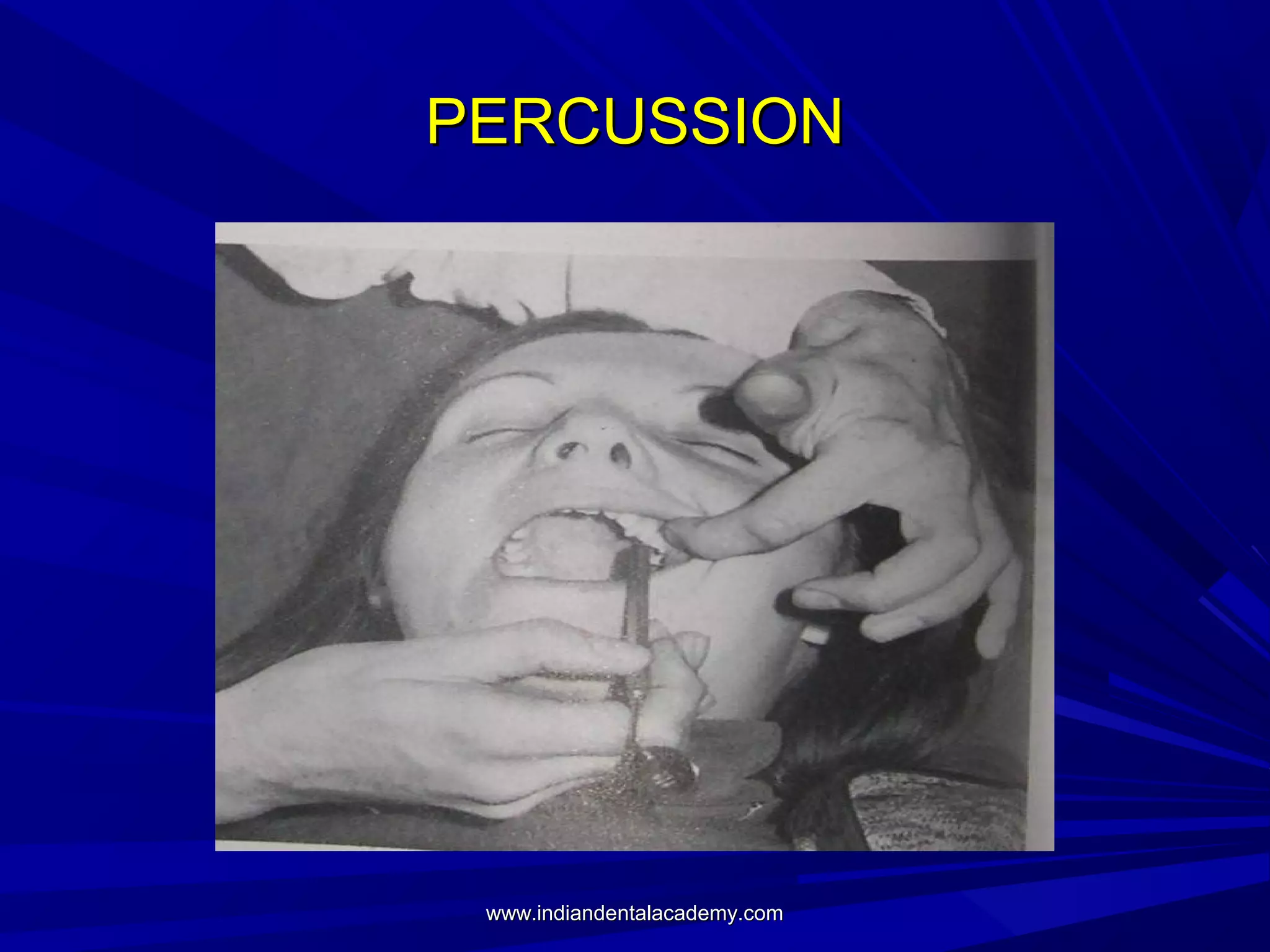
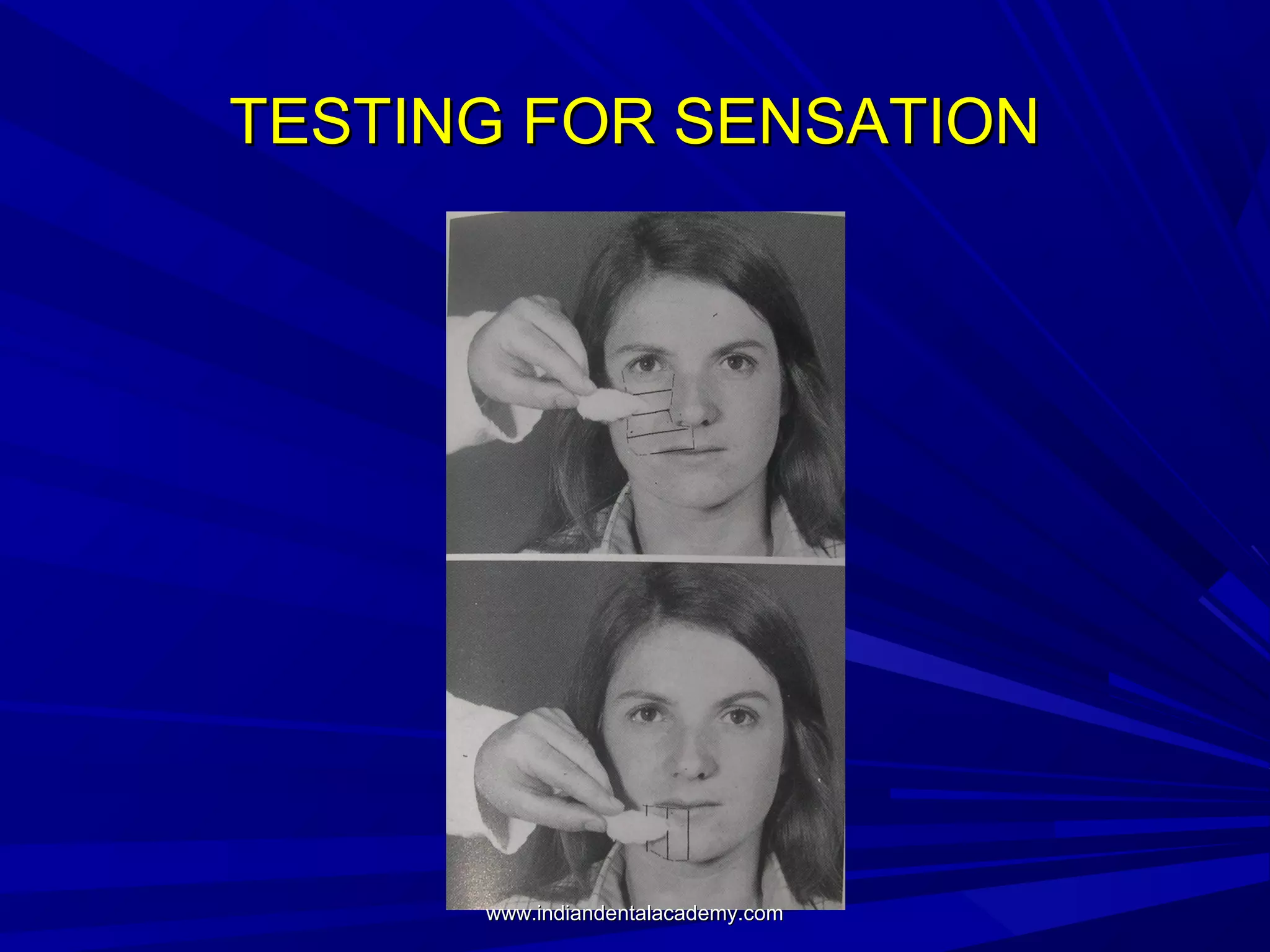
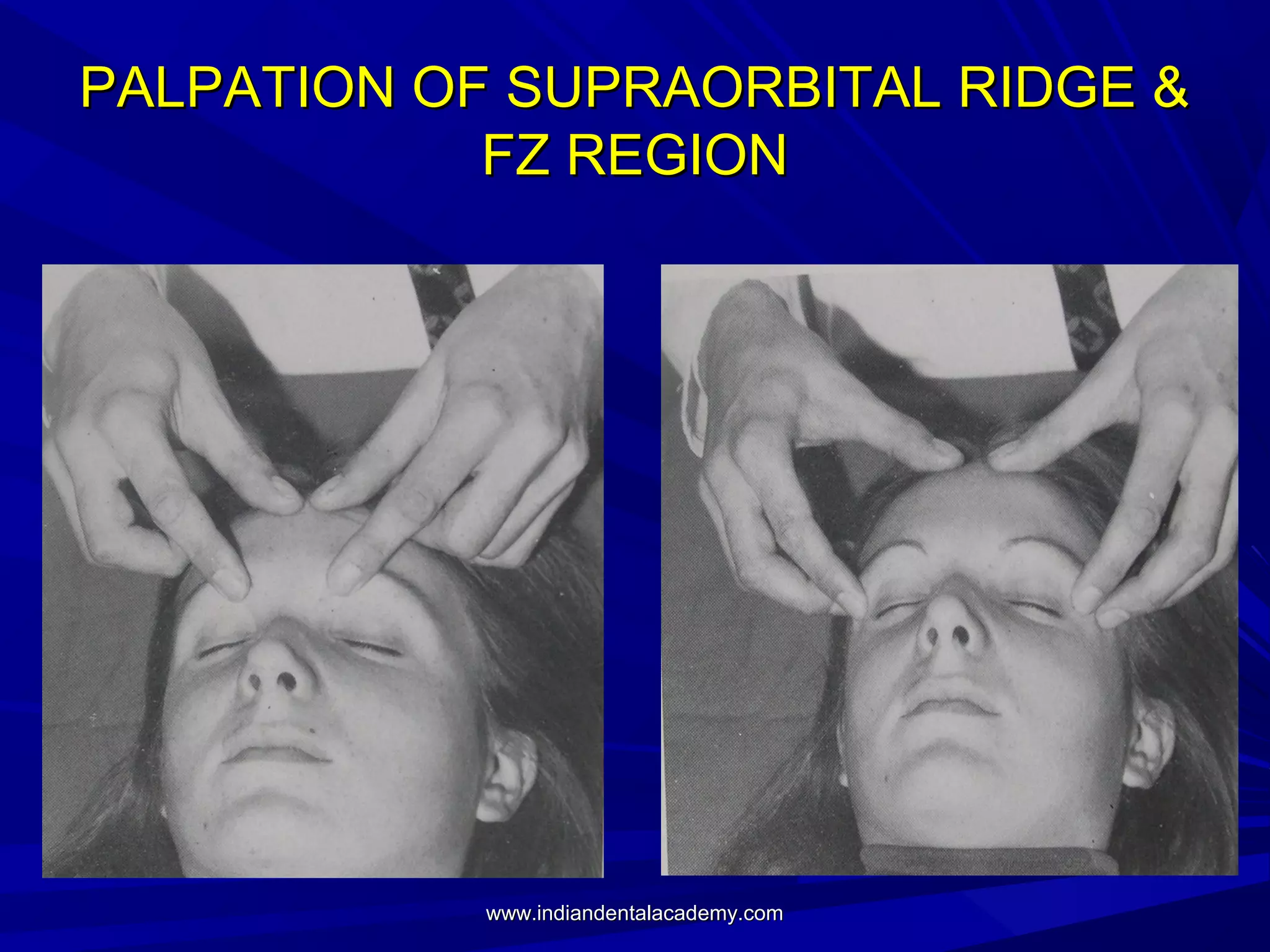
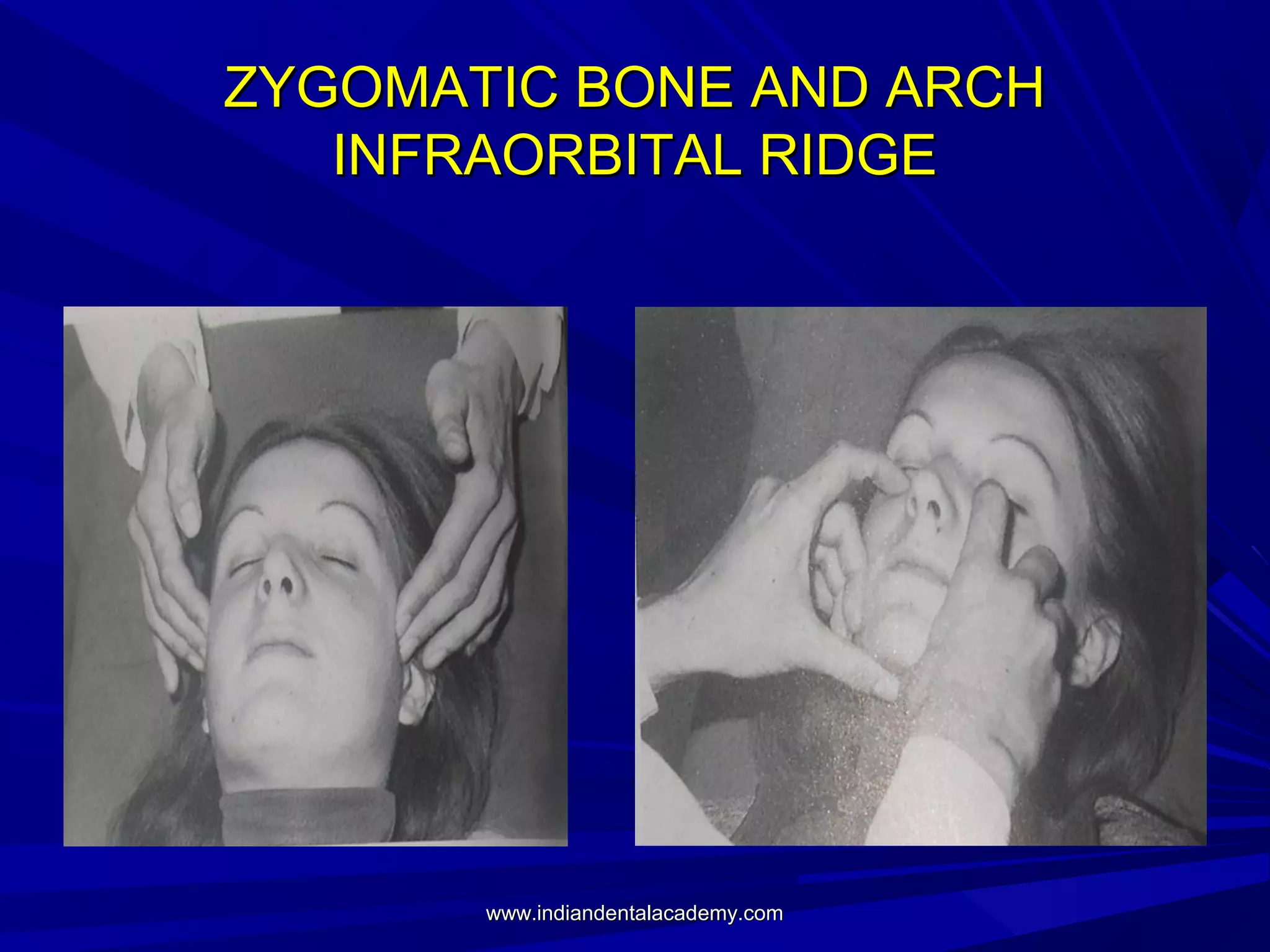
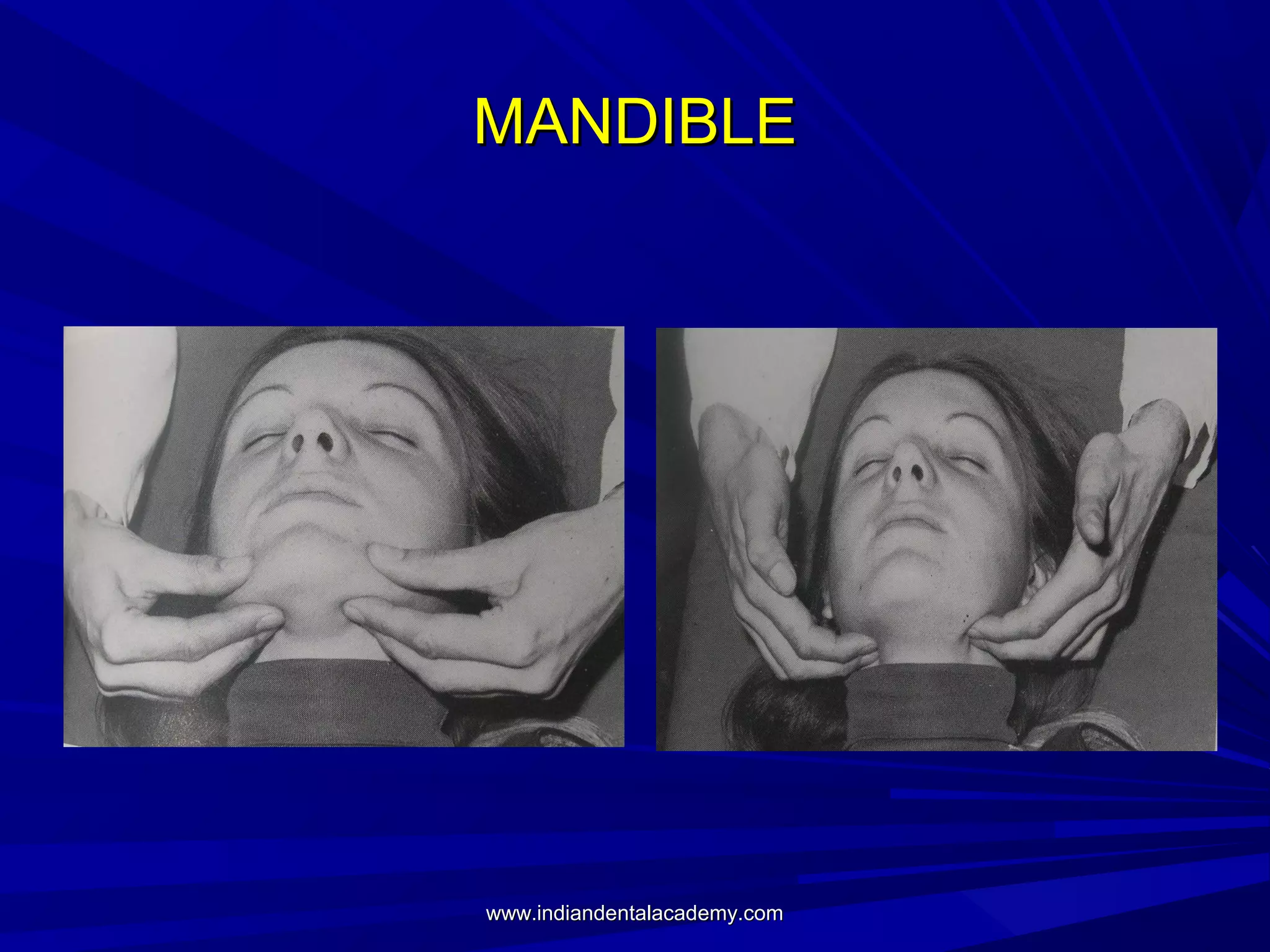
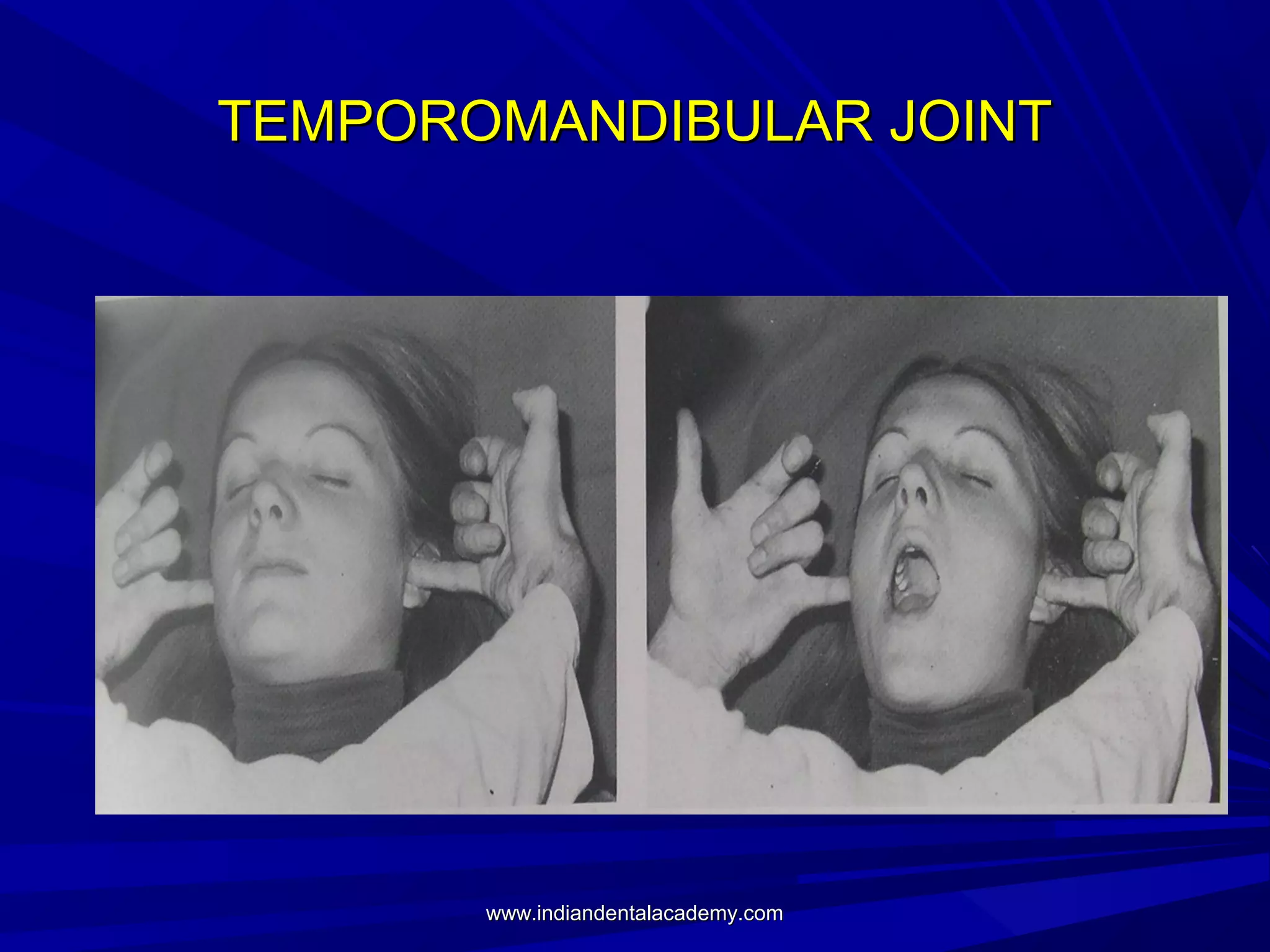


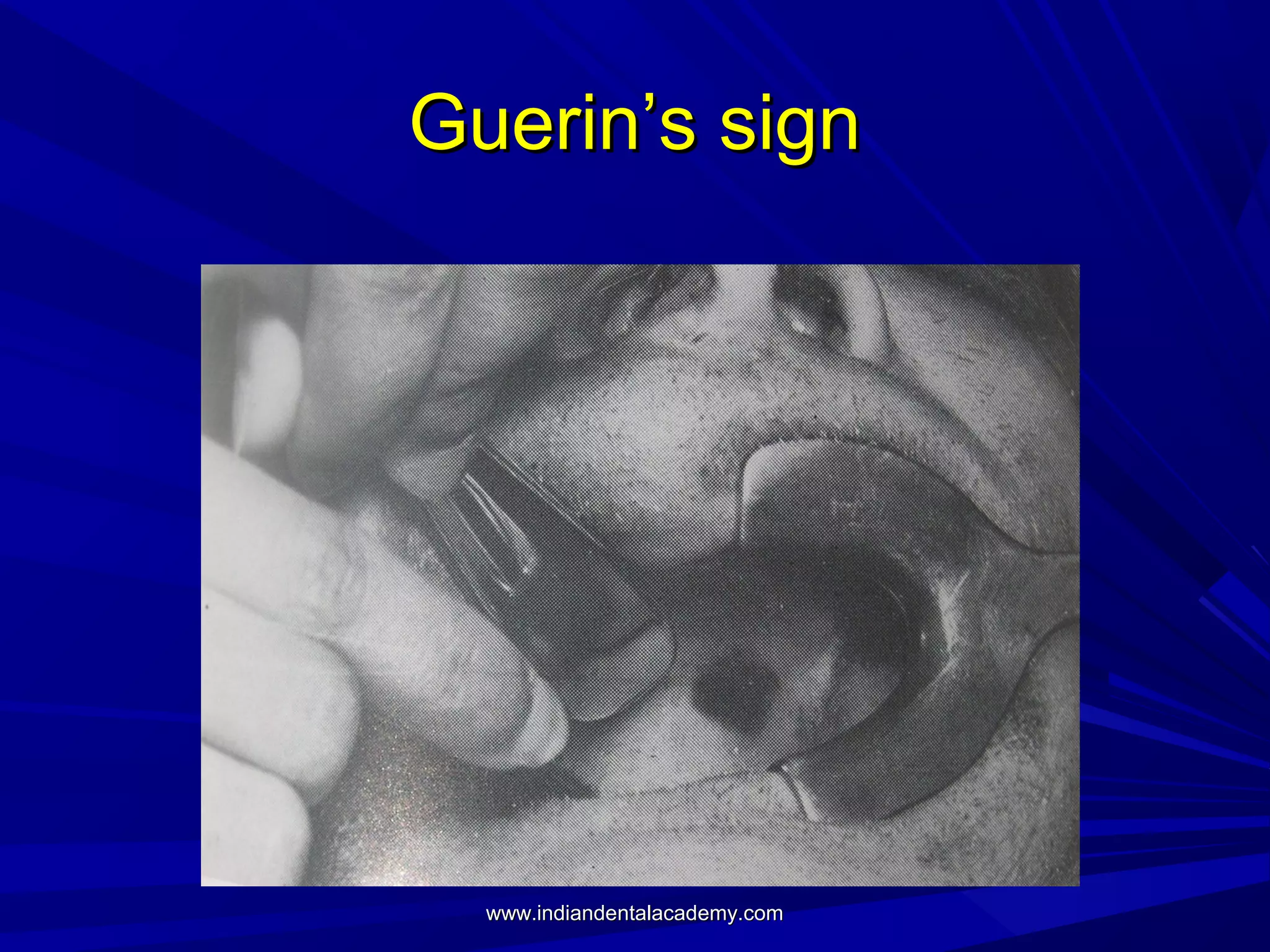


This document discusses the primary assessment and management of maxillofacial and head injuries. It outlines the steps in management including the primary and secondary surveys. The primary survey involves assessing the airway, breathing, circulation, disability and exposure. Specific injuries that can compromise breathing like flail chest and pneumothorax are discussed. Cervical spine injury is also a concern and proper immobilization is important. Diagnosis of maxillofacial injuries involves inspection, palpation and imaging. Secondary survey is a full head-to-toe examination to identify and treat all injuries.























































































