Learning objectives
• Defineabsolute stability
• Describe how the biological behavior of fractured bone is affected
by absolute stability
• Define indications for selection of absolute stability according to
AO principles
• Explain techniques for achieving absolute stability
2
3.
Bone fracture
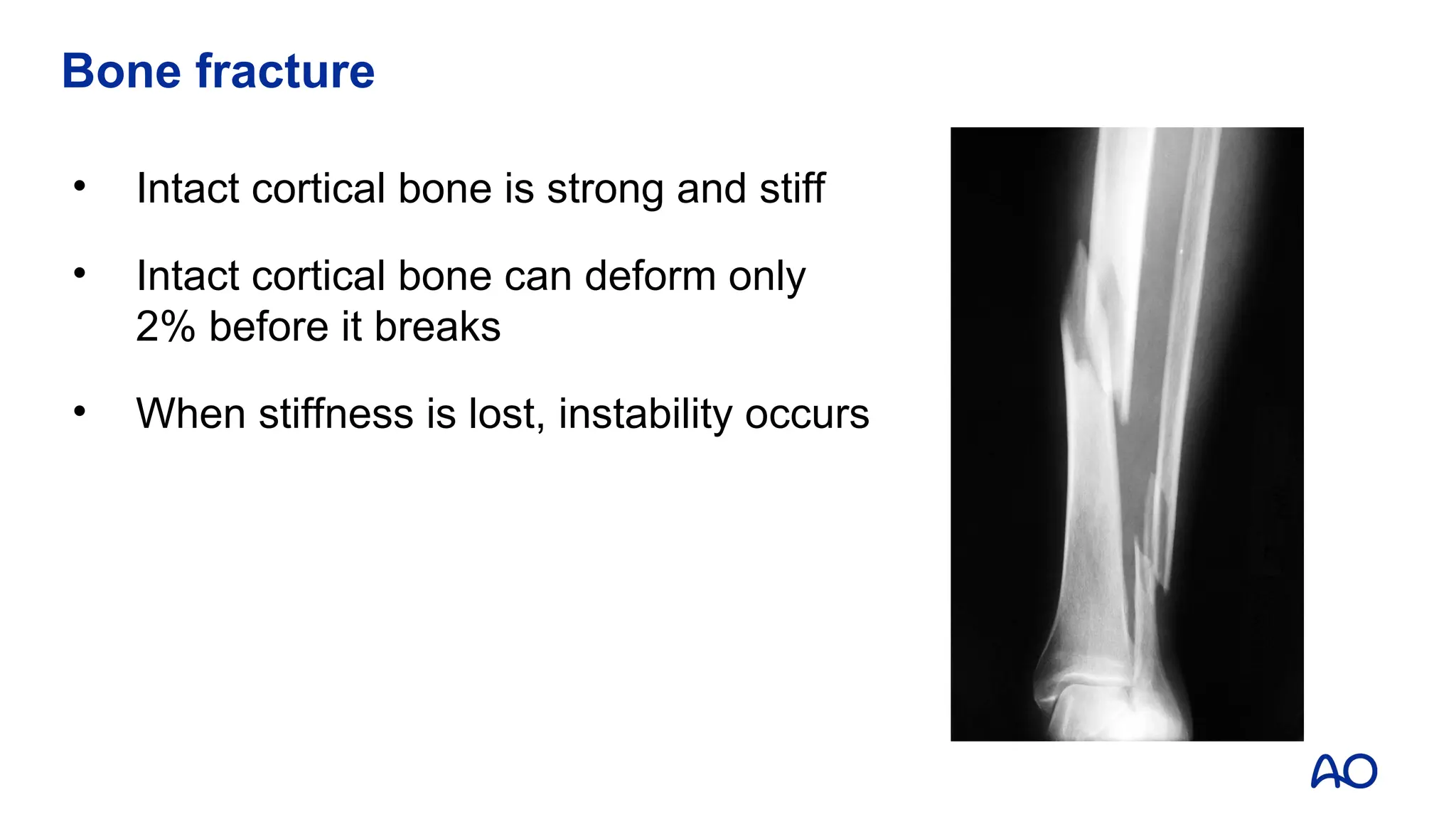
• Intactcortical bone is strong and stiff
• Intact cortical bone can deform only
2% before it breaks
• When stiffness is lost, instability occurs
4.
Fractured bone isdesigned to heal
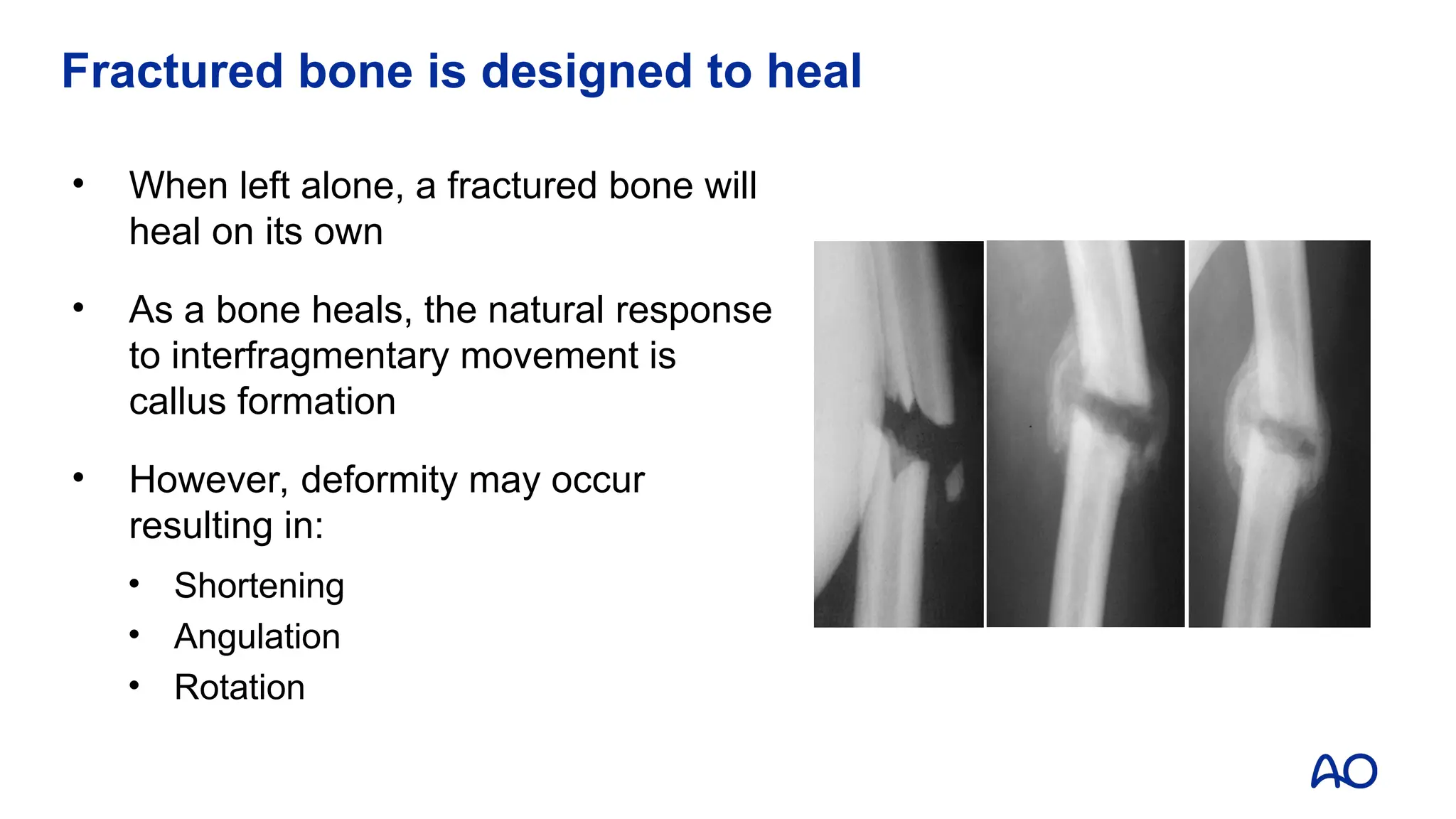
• When left alone, a fractured bone will
heal on its own
• As a bone heals, the natural response
to interfragmentary movement is
callus formation
• However, deformity may occur
resulting in:
• Shortening
• Angulation
• Rotation
5.
Aim of fracturetreatment
5
• Obtain and maintain reduction
• Restore stiffness (stability) for healing
• Decrease pain
• Promote healing
• Return of function
Degree of stability will determine the type
of bone healing
6.
How stability affectshealing
• Internal fixation of fractures alters the biology of fracture healing
• Method of bone healing depends on:
• Type of fracture (simple or complex)
• Type of reduction (anatomical or functional)
• Type of stability achieved (absolute or relative)
• Type of implant chosen (providing absolute or relative
stability)
7.
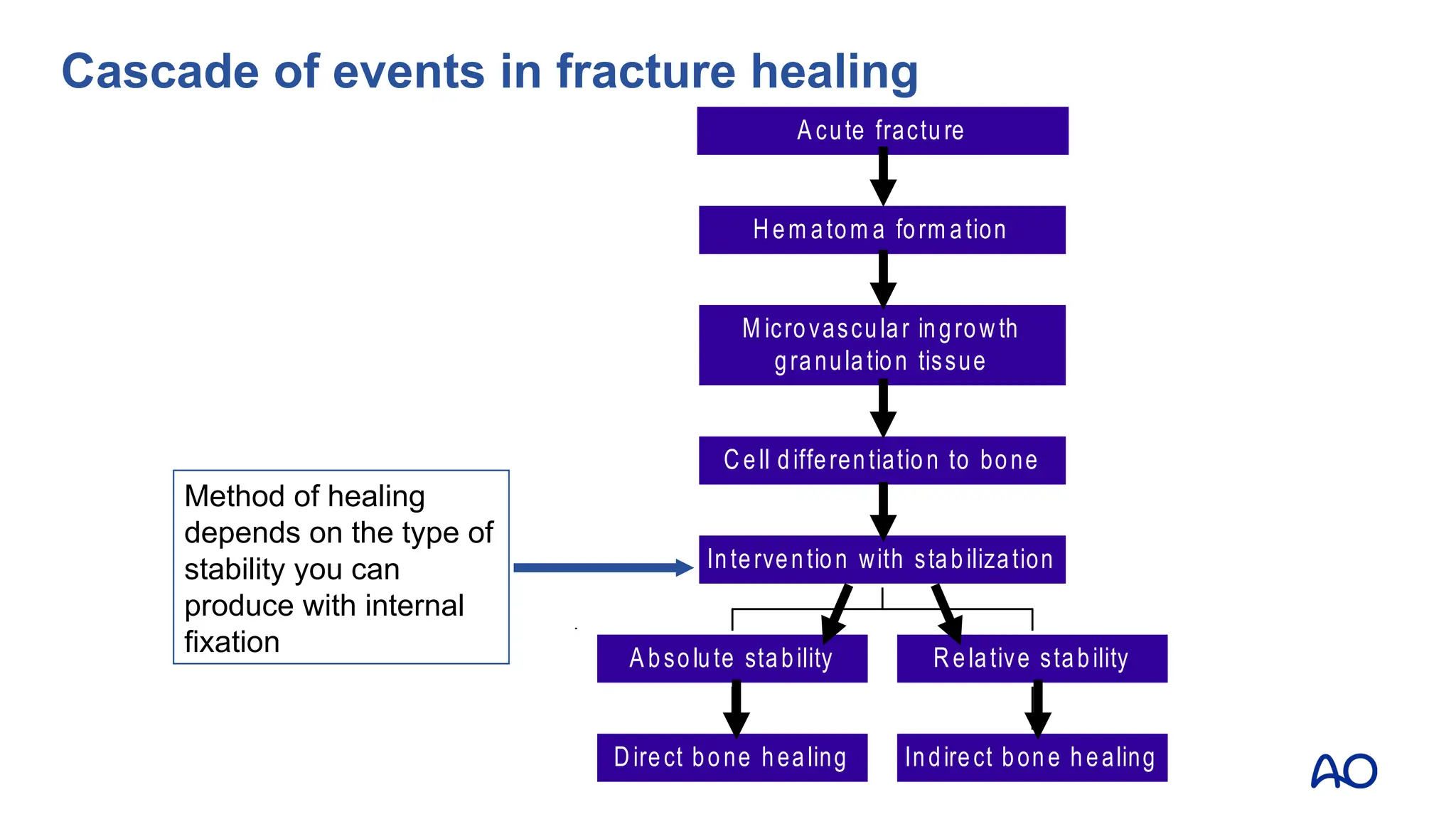
Direct bone healing
Absolute stability
Indirect bone healing
Relative stability
Intervention with stabilization
Cell differentiation to bone
M icrovascular ingrowth
granulation tissue
Hem atom a form ation
A cute fracture
Method of healing
depends on the type of
stability you can
produce with internal
fixation
Cascade of events in fracture healing
8.
Definition of absolutestability
• Absolute stability means that there is no micro-motion at the
fracture site under normal physiological loads
• This requires open reduction
• This requires anatomical reduction of the fracture
• Best method to produce absolute stability is with interfragmentary
compression
• Absolute stability usually leads to direct bone healing
8
9.
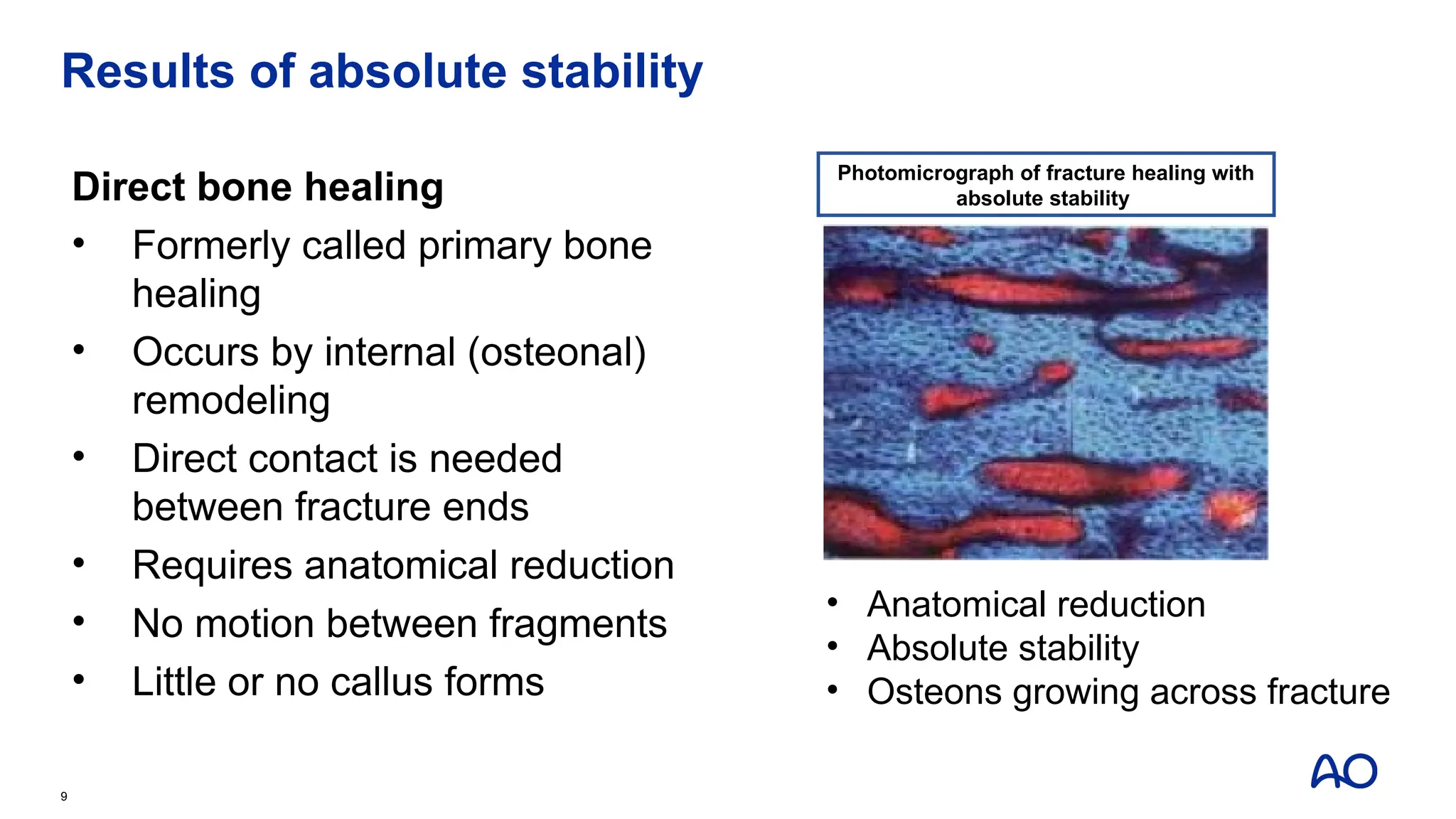
Results of absolutestability
Direct bone healing
• Formerly called primary bone
healing
• Occurs by internal (osteonal)
remodeling
• Direct contact is needed
between fracture ends
• Requires anatomical reduction
• No motion between fragments
• Little or no callus forms
9
• Anatomical reduction
• Absolute stability
• Osteons growing across fracture
Photomicrograph of fracture healing with
absolute stability
10.
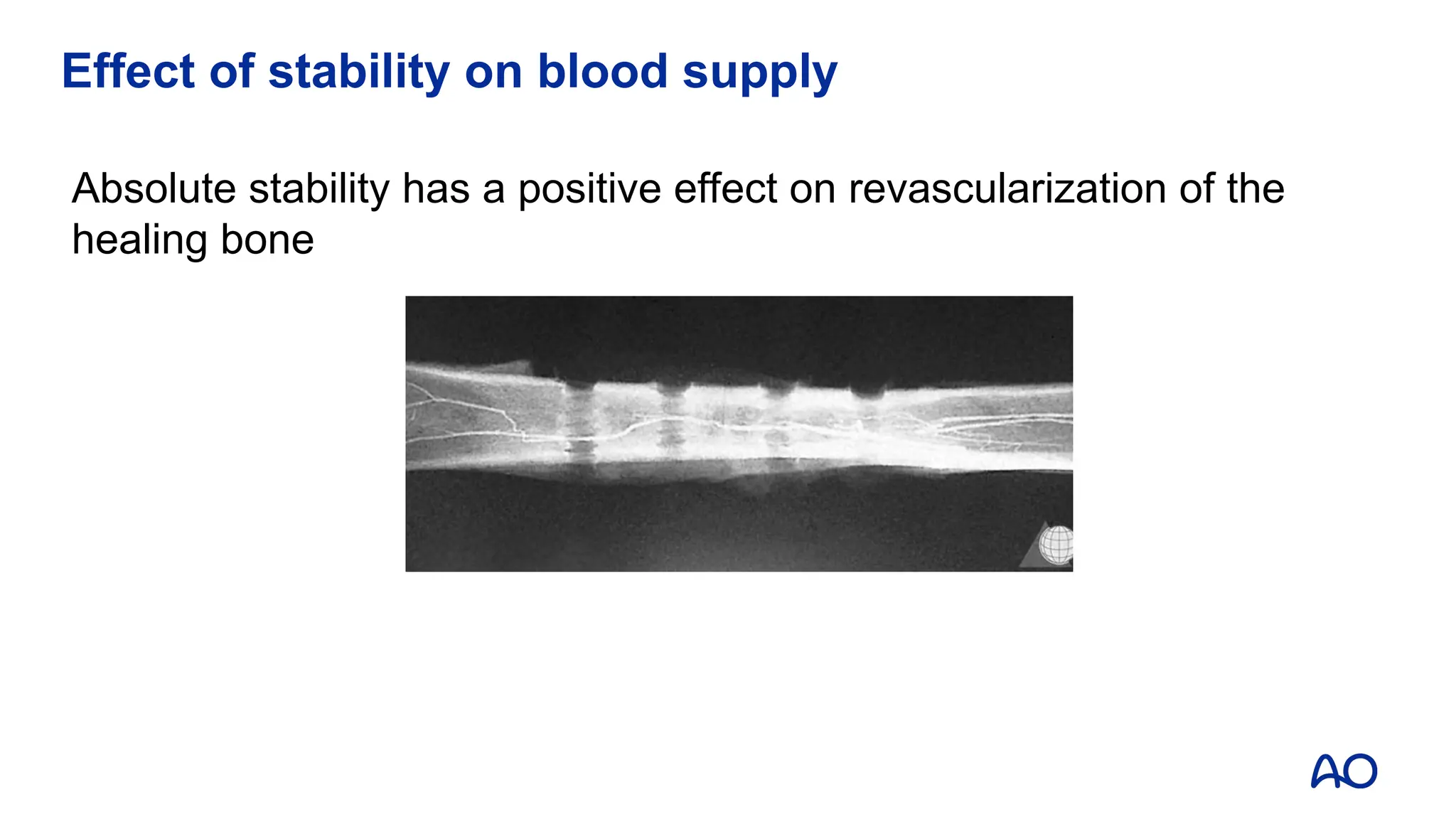
Effect of stabilityon blood supply
Absolute stability has a positive effect on revascularization of the
healing bone
11.
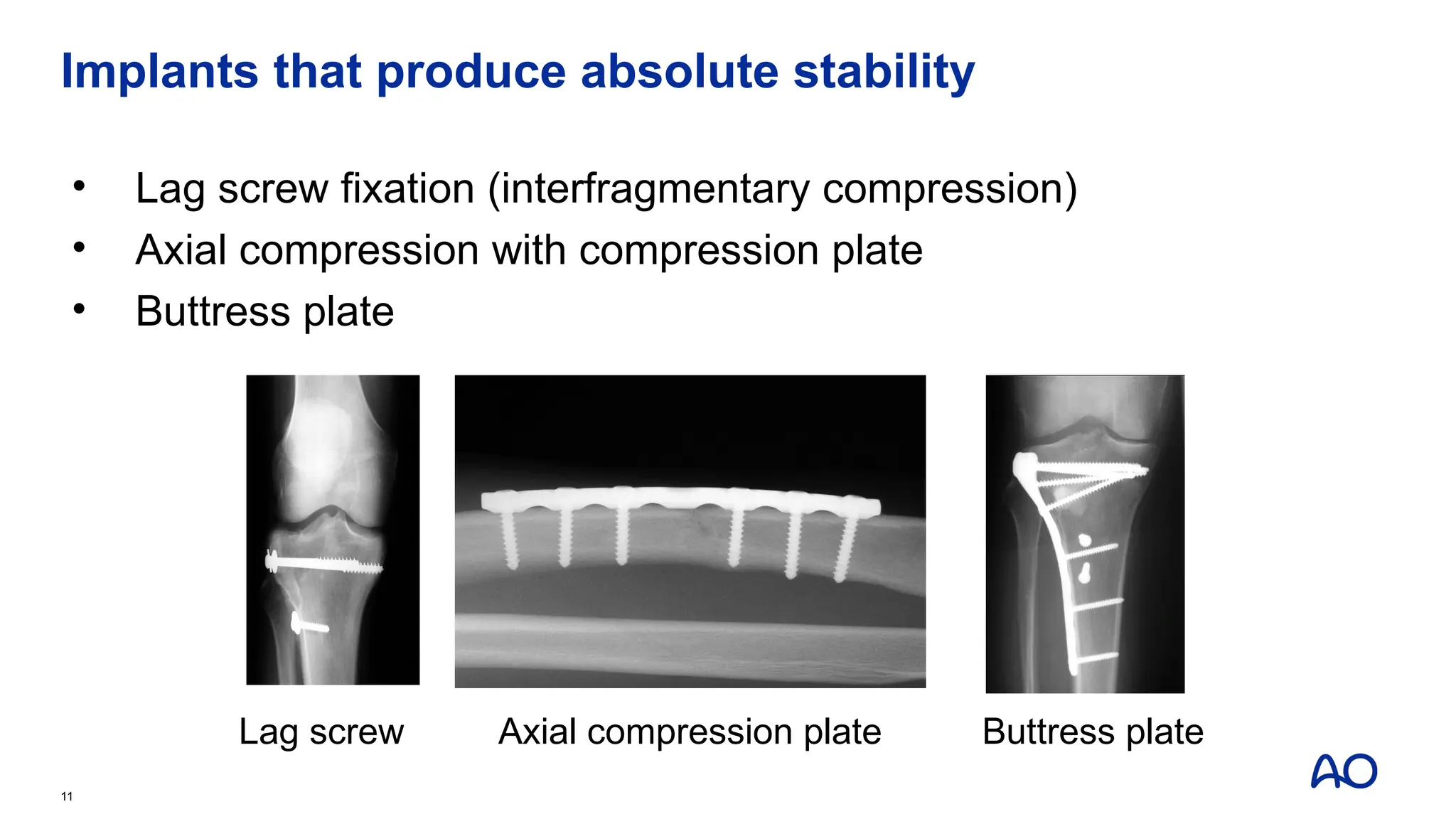
Implants that produceabsolute stability
• Lag screw fixation (interfragmentary compression)
• Axial compression with compression plate
• Buttress plate
11
Lag screw Axial compression plate Buttress plate
12.
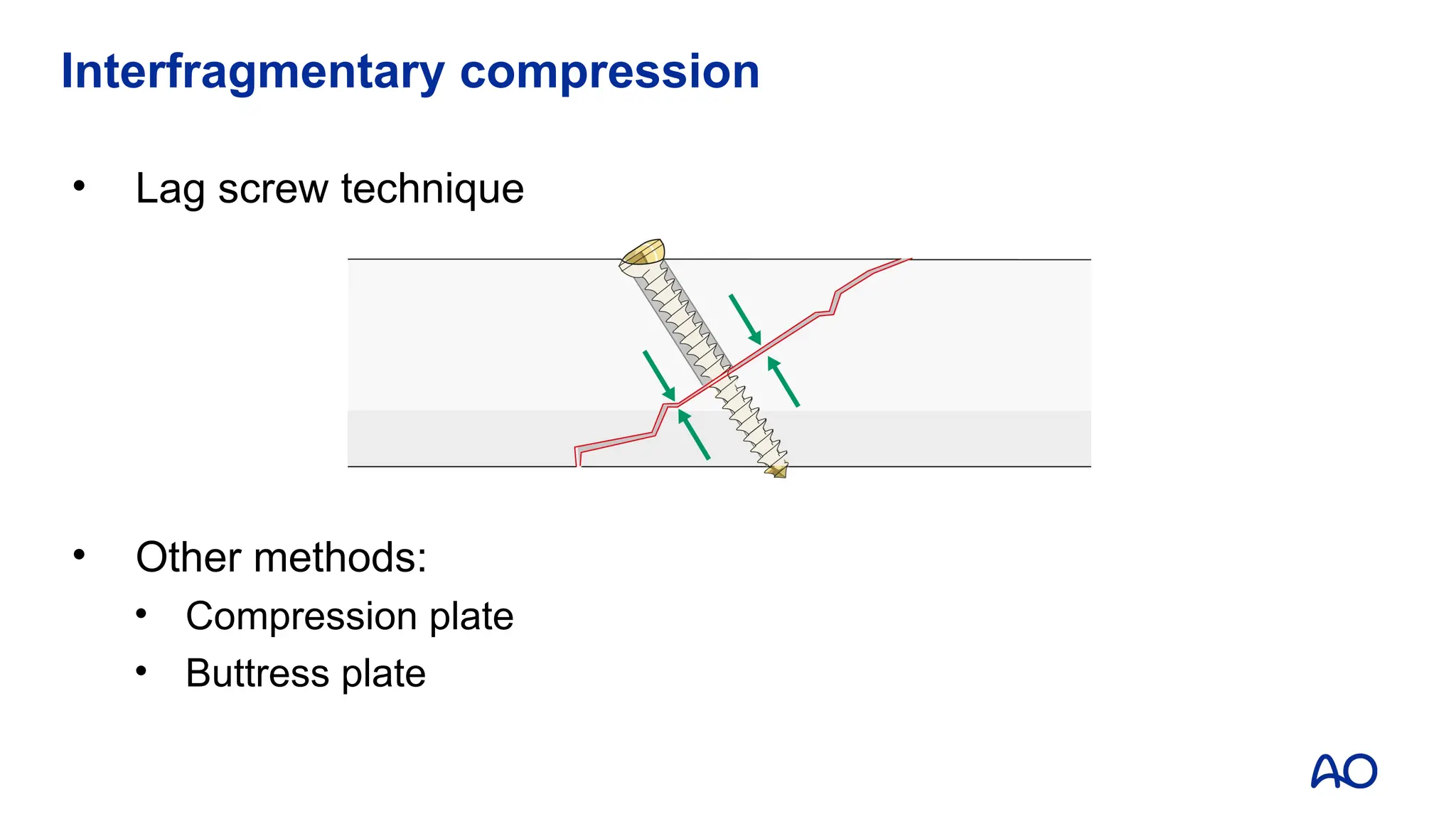
Lag screw fixation
•Lag screw is a technique, not a type of screw
• Any screw can function as a lag screw to provide
interfragmentary compression if it is inserted properly
• Shaft screw is the only screw that is designed as a lag screw to
provide interfragmentary compression
12
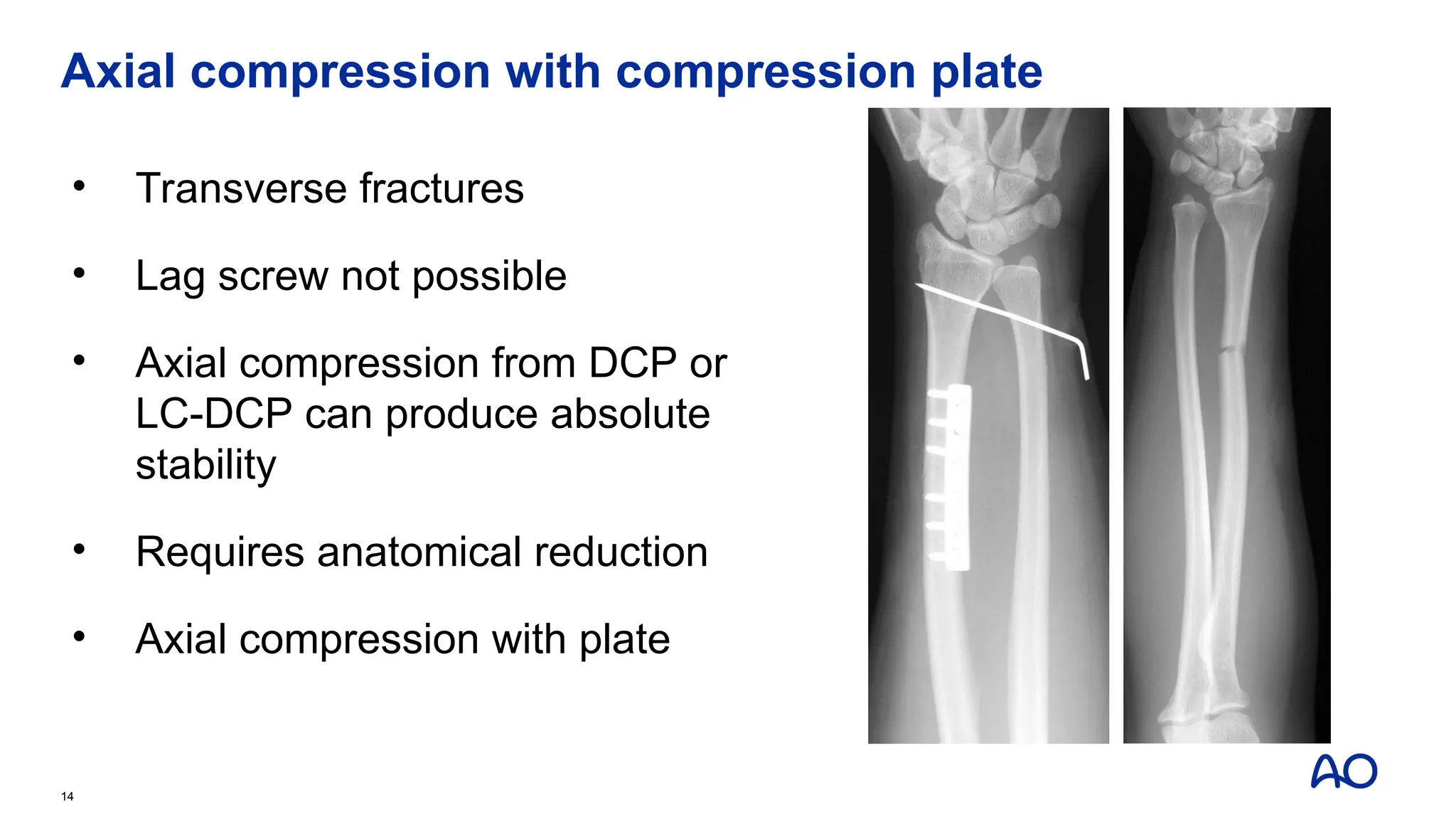
Axial compression withcompression plate
• Transverse fractures
• Lag screw not possible
• Axial compression from DCP or
LC-DCP can produce absolute
stability
• Requires anatomical reduction
• Axial compression with plate
14
15.
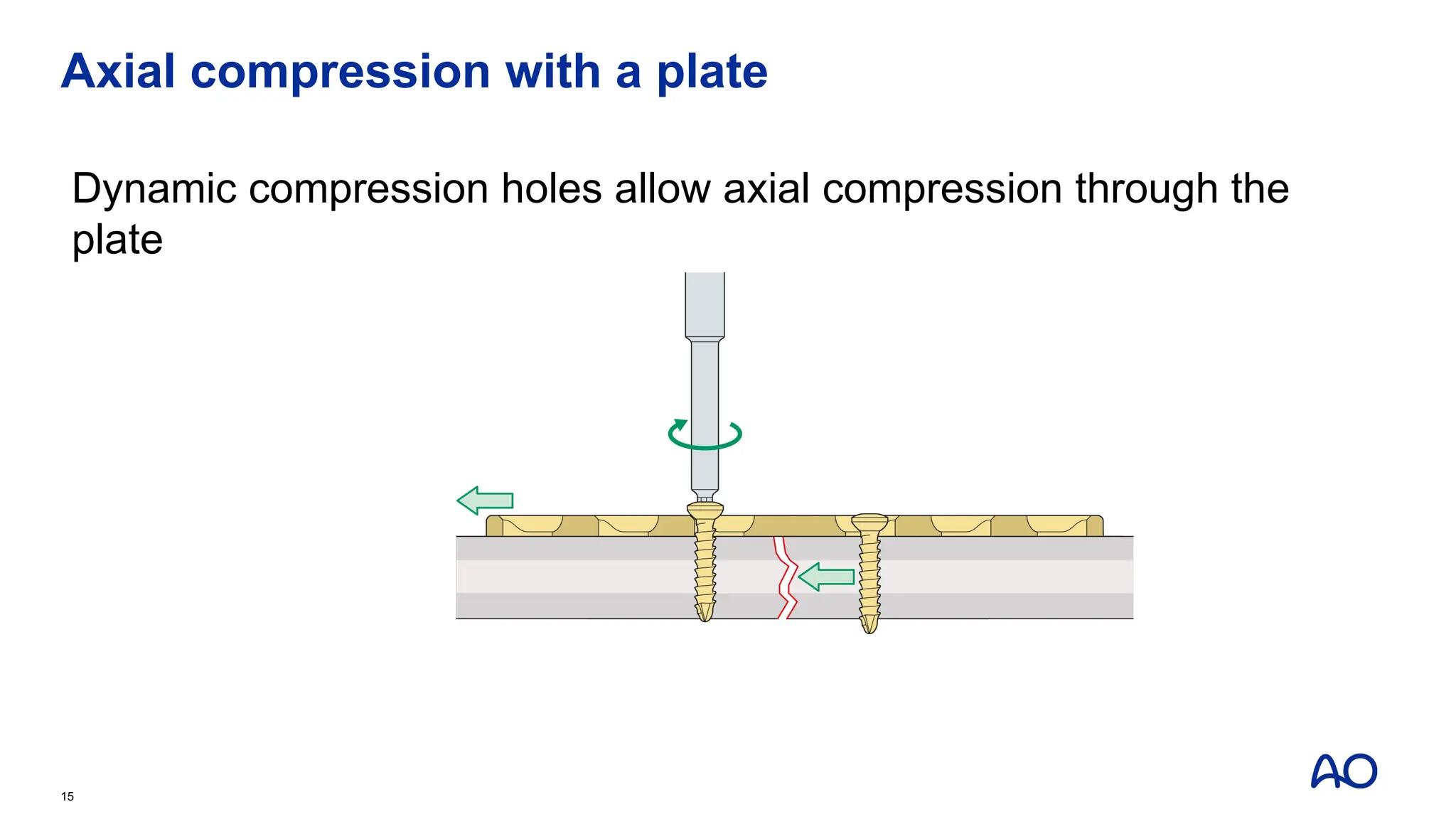
Axial compression witha plate
Dynamic compression holes allow axial compression through the
plate
15
16.
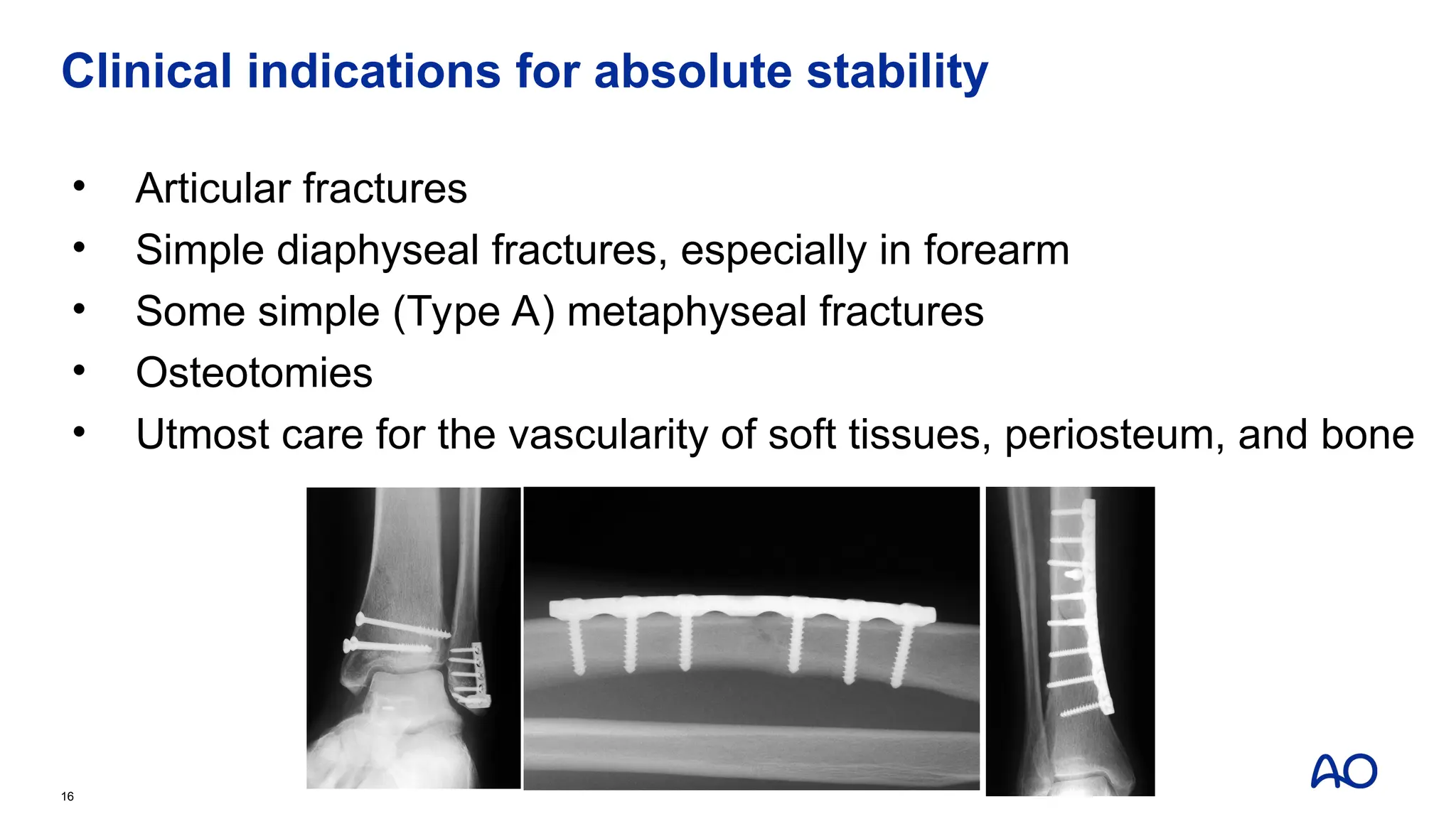
Clinical indications forabsolute stability
• Articular fractures
• Simple diaphyseal fractures, especially in forearm
• Some simple (Type A) metaphyseal fractures
• Osteotomies
• Utmost care for the vascularity of soft tissues, periosteum, and bone
16
17.
Principles of thelag screw technique
• It is a technique of insertion, not a type of screw
• Any screw can function as a lag screw
• A lag screw produces interfragmentary compression
• A lag screw can produce up to 2,500–3,000 Newtons of force
• Lag screw fixation will result in absolute stability
18.
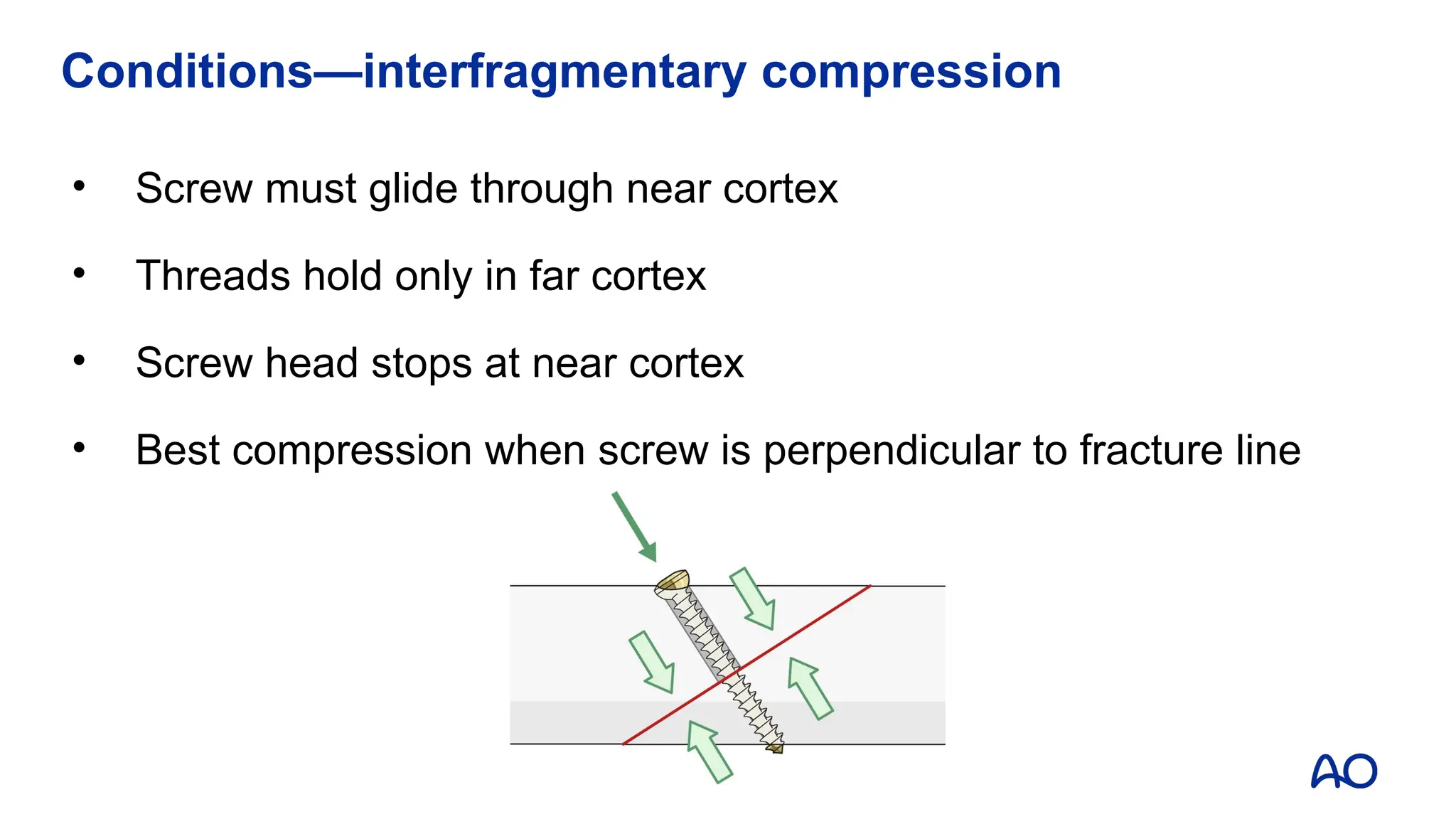
• Screw mustglide through near cortex
• Threads hold only in far cortex
• Screw head stops at near cortex
• Best compression when screw is perpendicular to fracture line
Conditions—interfragmentary compression
19.
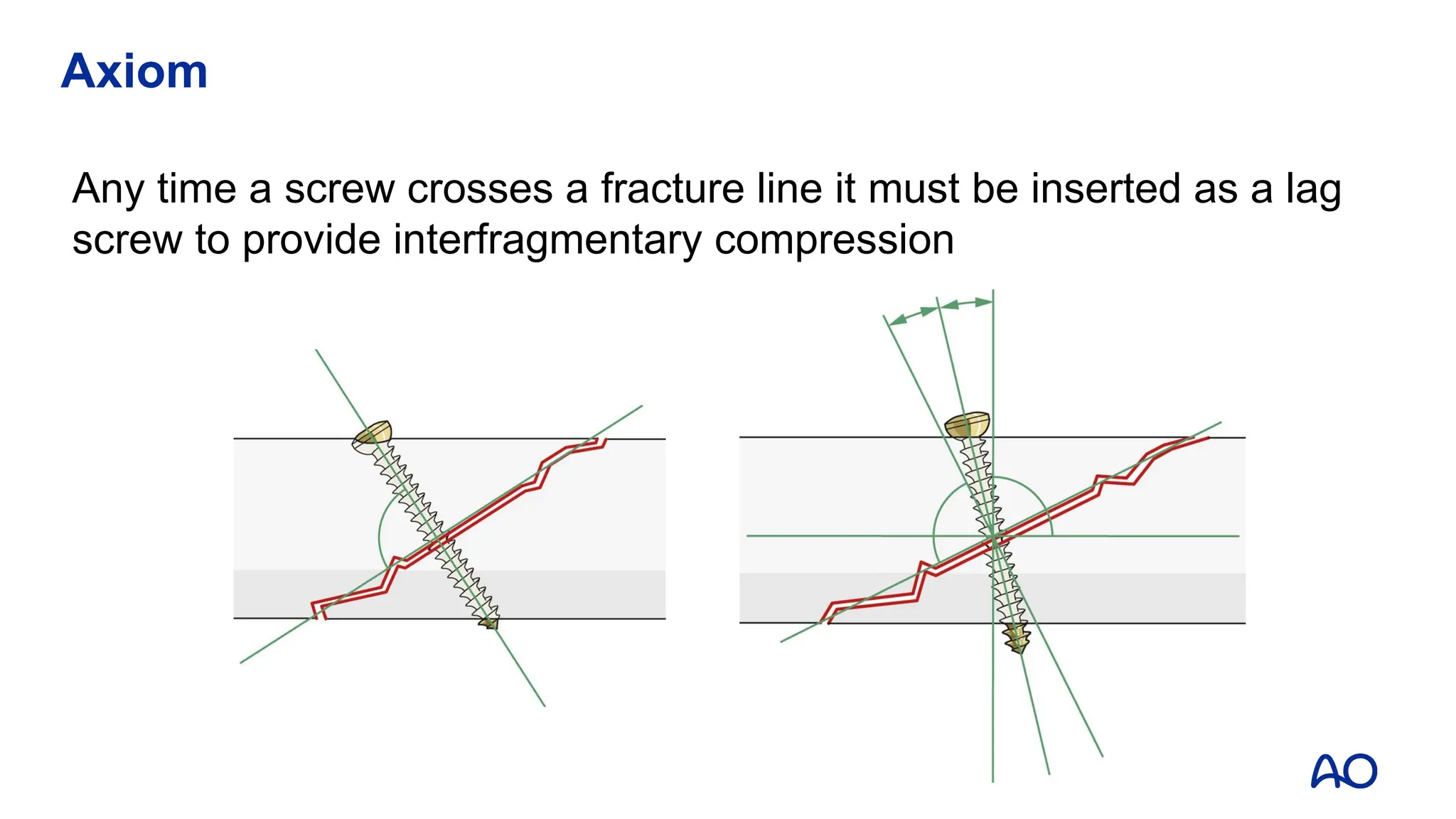
Axiom
Any time ascrew crosses a fracture line it must be inserted as a lag
screw to provide interfragmentary compression
20.
Take-home messages
• Absolutestability implies there is no motion between fracture fragments
with normal functional loads
• The best method to achieve absolute stability is with interfragmentary
compression (lag screw technique)
• Absolute stability is indicated for articular fractures and simple
diaphyseal fractures
• Fractures treated with absolute stability can be expected to heal with
direct bone healing with no callus
20
Editor's Notes
#1 Published: July 2013
Author: Steven Schelkun
Revised: 2018
Reviewer: Wael Taha
#2 Teaching points:
Consider the spectrum of stability.
#3 Photo courtesy of Steven R Schelkun, MD
The important mechanical characteristics of cortical bone are stiffness and strength.
Bone is a strong material but it breaks under very little deformation (2%).
When a mechanical load or force is applied to an intact bone that exceeds the structural integrity of the bone, a fracture will occur.
A fractured bone produces instability.
#4 I think we can all agree that a fractured bone produces some degree of instability.
However, when left alone, a fractured bone will most likely heal on its own.
As a bone heals, the natural response to interfragmentary movement is callus formation.
However, without some type of stability during healing process, deformity may occur such a shortening, angulation or rotation.
#7 Diagram courtesy of Steven R Schelkun, MD
A surgeon has the option of intervening with surgical stabilization of a fracture.
Internal fixation of fractures alters the biology of fracture healing.
The type of fixation applied and the amount of stability achieved will determine the type of bone healing that will occur.
#9 Photomicrograph:
This shows a photomicrograph of an osteotomy that has been anatomically reduced and stably fixed with absolute stability. You can see the cutting cones with osteons crossing the fracture line. This is a good example of direct bone healing.
#10 References:
Schenk R and Willenegger H, 1963 (Title? Citation by author in PubMed is probably not the right one.)
Under stable conditions, blood vessels may cross a fracture site more easily. Absolute stability supports the repair and early revascularization of the fracture site.
The callus in the image does not look like callus from instability but rather periosteal callus at the end of the plate or from periosteal stripping from the osteotomy. If this were callus from relative stability you would expect to also see resorption at the fracture site and an accumulation of "bridging callus" at the fracture site, and consequently the endosteal canal would be filed with callus and fibrocartilage and there would be no patent blood vessels crossing the fracture.
#11 Photo courtesy of Steven R Schelkun, MD
Examples of lag screw fixation, axial compression with a compression plate, and a buttress plate all producing absolute stability.
#12 It is important to remember that lag screw is a technique, not a type of screw.
Any screw can function as a lag screw depending on how it is inserted.
A shaft screw is the only screw that is specifically designed as a lag screw to provide interfragmentary compression.
#13 Illustration courtesy of AO Manual
The best method to produce interfragmentary compression is the lag screw technique.
Other methods that may produce absolute stability include an axial compression plate or a buttress plate.
The amount of compressive preload from these last two methods are not nearly as great as with the lag screw technique.
#14 A lag screw provides maximum compression when the screw is perpendicular to the fracture line.
Some fracture configurations, however, are transverse and will not accept a lag screw.
In this case a DCP or LC-DCP can be used to provide axial compression and achieve absolute stability.
This technique requires anatomical reduction of the fracture and axial compression using the dynamic compression holes of the implant.
This example shows a Galeazzi fracture with a transverse fracture of the radius and disruption of the distal radio-ulnar joint.
At six weeks this fracture shows evidence of healing across the fracture line with no callus formation. This is just prior to pin removal of the distal radio-ulnar joint.
#16 The indications for producing absolute stability depend on specific types of fractures.
These include articular fractures, simple forearm fractures, and simple (type A) metaphyseal fractures.
No matter what fracture is treated, the surgeon must maintain the utmost care for the vascularity of the soft tissues, periosteum in bone.
#17 The lag screw principle is one of the most important concepts of internal fixation.
Any screw can function as a lag screw.
The application of a lag screw is a technique of how a screw is inserted, not a type of screw.
A lag screw provides interfragmentary compression between two bone fragments.
This type of screw can produce up to 3,000 N of force between the bone fragments.
Leg screw fixation will usually results in absolute stability.
#18 In order for the lag screw technique to work, certain conditions must apply:
-The screw must glide through the cortex immediately beneath the screw head.
-The threads of the screw obtain purchase only in the far cortex.
-The under surface of the screw head must stop at the near cortex.
-Maximum interfragmentary compression occurs when the screw is oriented perpendicular to the fracture line.
#19 An important axiom of internal fixation indicates that any time a screw crosses a fracture line, it must be inserted as a lag screw to provide interfragmentary compression.