Downloaded 14 times






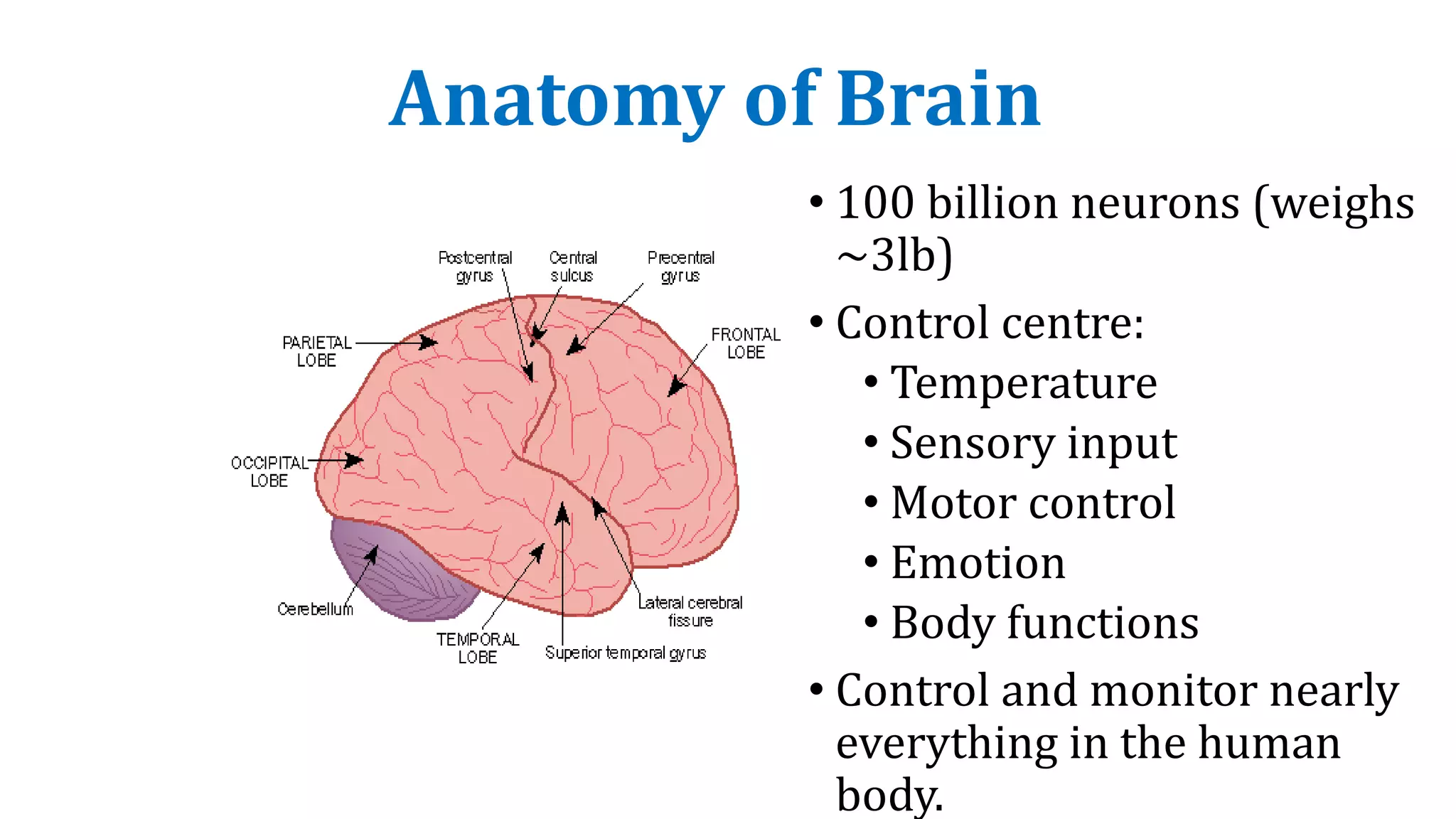
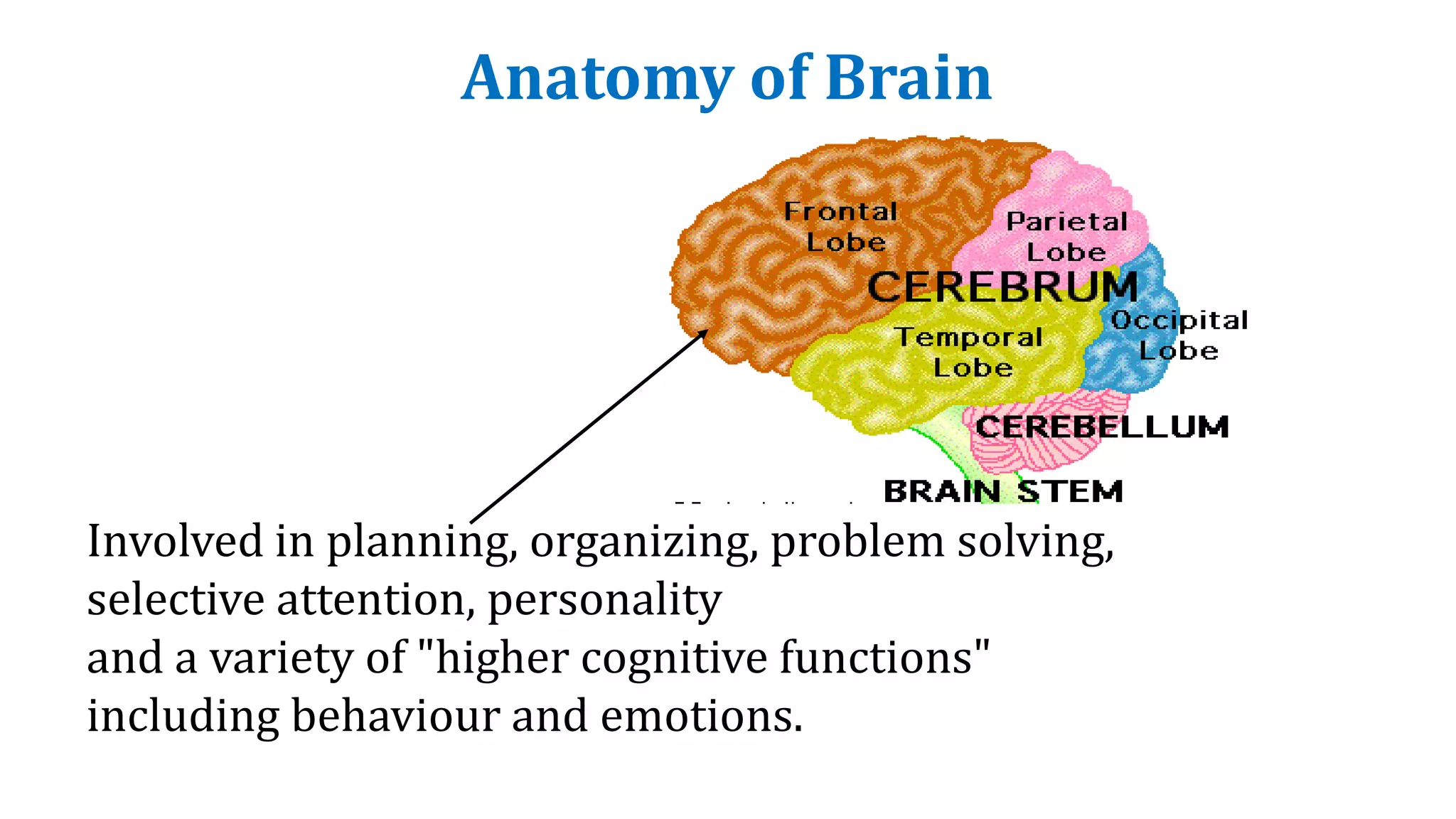




















































The document discusses epilepsy and antiseizure drugs. It defines epilepsy as a neurological disorder involving recurrent seizures. It describes the anatomy of the brain, common triggers for seizures, classification of seizures, and drugs commonly used to treat epilepsy such as carbamazepine, valproate, phenytoin, and levetiracetam. Optimum treatment involves using one drug initially and increasing the dose gradually while monitoring for side effects and therapeutic drug levels.



































































