More Related Content
Similar to Antibiotic dosing in msof.full
Similar to Antibiotic dosing in msof.full (20)
Recently uploaded
Industrial Policy - 1948, 1956, 1973, 1977, 1980, 1991Industrial Policy - 1948, 1956, 1973, 1977, 1980, 1991RKavithamani
Antibiotic dosing in msof.full
- 1. Antibiotic Dosing in Multiple Organ
Dysfunction Syndrome
Marta Ulldemolins, Jason A. Roberts, Jeffrey Lipman and Jordi Rello
Chest 2011;139;1210-1220
DOI 10.1378/chest.10-2371
The online version of this article, along with updated information and
services can be found online on the World Wide Web at:
http://chestjournal.chestpubs.org/content/139/5/1210.full.html
Chest is the official journal of the American College of Chest
Physicians. It has been published monthly since 1935.
Copyright2011by the American College of Chest Physicians, 3300
Dundee Road, Northbrook, IL 60062. All rights reserved. No part of
this article or PDF may be reproduced or distributed without the prior
written permission of the copyright holder.
(http://chestjournal.chestpubs.org/site/misc/reprints.xhtml)
ISSN:0012-3692
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
© 2011 American College of Chest Physicians
- 2. CHEST Postgraduate Education Corner
CONTEMPORARY REVIEWS IN CRITICAL CARE MEDICINE
Antibiotic Dosing in Multiple Organ
Dysfunction Syndrome
Marta Ulldemolins, PharmD; Jason A. Roberts, PhD, BPharm(Hons); Jeffrey Lipman, MD;
and Jordi Rello, MD, PhD
Although early and appropriate antibiotic therapy remains the cornerstone of success for the
treatment of septic shock, few data exist to guide antibiotic dose optimization in critically ill
patients, particularly those with multiple organ dysfunction syndrome (MODS). It is well known
that MODS significantly alters the patient’s physiology, but the effects of these variations on phar-
macokinetics have not been reviewed concisely. Therefore, the aims of this article are to sum-
marize the disease-driven variations in pharmacokinetics and pharmacodynamics and to provide
antibiotic dosing recommendations for critically ill patients with MODS. The main findings of this
review are that the two parameters that vary with greatest significance in critically ill patients
with MODS are drug volume of distribution and clearance. Disease- and clinician-driven changes
lead to an increased volume of distribution and lower-than-expected plasma drug concentrations
during the first day of therapy at least. Decreased antibiotic clearance is common and can lead
to drug toxicity. In summary, “front-loaded” doses of antibiotic during the first 24 h of therapy
should account for the likely increases in the antibiotic volume of distribution. Thereafter, main-
tenance dosing must be guided by drug clearance and adjusted to the degree of organ dysfunction.
CHEST 2011; 139(5):1210–1220
Abbreviations: AKI 5 acute kidney injury; AUC0-24 5 area under the concentration curve over 0 to 24 h; CL 5 clearance;
Cmax 5 peak concentration; CrCL 5 creatinine clearance; ƒ T . MIC 5 time over minimum inhibitory concentration;
GFR 5 glomerular filtration rate; MDRD 5 modified diet in renal disease; MIC 5 minimum inhibitory concentration;
MODS 5 multiple organ dysfunction syndrome; PK/PD 5 pharmacokinetic/pharmacodynamic; RRT 5 renal replacement
therapy; TDM 5 therapeutic drug monitoring; Vd 5 volume of distribution
Despiteuse, treatment of severe infections remains
biotic
decades of clinical experience with anti- however, there is an absence of guidance on rational
approaches to antibiotic dosing in patients with mul-
a challenge for clinicians. Over the past years, two tiple organ dysfunction syndrome (MODS) who have
important phenomena have made even more essen- higher levels of sickness severity and whereby effec-
tial the need to improve the use of presently available tive antibiotic therapy may be even more important
antibiotics and to extend the effective life of a drug: to clinical outcome. The purpose of this article is to
(1) the escalation in the incidence of bacteria resis- review, using examples from the literature, the key con-
tant to the available antibiotics1 and (2) the dearth of cepts likely to affect antibiotic pharmacokinetics and
antimicrobial drugs with new mechanisms of action pharmacodynamics and to provide dose recommen-
in development.2 One mechanism to improve optimi- dations for the treatment of critically ill patients with
zation of antibiotic use may be improvement of anti- MODS.
biotic dosing because a causal relationship is thought
to exist among inappropriate dosing, clinical out- Search Strategy and Selection Criteria
come, and the development of bacterial resistance.3
From a clinical perspective, optimization of antibiotic Data were identified by a systematic search in
use is particularly important for critically ill patients in PubMed (1966-October 2010) for original articles
whom early and appropriate antibiotic prescription that evaluated the variations in antibiotic pharmaco-
has been shown to reduce mortality.4-10 The physio- kinetics and pharmacokinetics/pharmacodynamics
logic and pharmacokinetic derangements in antibiotics (PK/PD) in MODS. Key words used were “sepsis” or
have been reviewed previously for patients with sepsis11; “systemic inflammation response syndrome” or “septic
1210 Postgraduate Education Corner
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
© 2011 American College of Chest Physicians
- 3. shock” or “multiple organ failure” and “antibacterial lent to the extracellular water and usually corresponds
agents” or “antibiotics” and “pharmacokinetics” or to a value between 0.1 L/kg and 0.3 L /kg.11 On the con-
“pharmacodynamics” and “critically ill patient” or trary, lipophilic drugs can cross lipid membranes and,
“intensive care unit” or “critical care.” A total of therefore, distribute intracellularly and into adipose
167 articles were returned, of which only 48 were tissues. Hence, the Vd of lipophilic drugs depends
deemed relevant for critically ill patients with MODS on the amount of adipose tissue, which generally is
or some level of organ dysfunction. Numerous articles proportional to total body weight.11 There are a few
also were identified through searches of the exten- exceptions where this approach cannot be extrapo-
sive files of the authors. lated, for example, in patients with increased muscle
mass, as muscle tissue is highly hydrophilic and
affects the Vd of lipophilic drugs to a lesser extent.
Overview of Antibiotic Physicochemistry,
Pharmacokinetics, and Pharmacodynamics
Pharmacokinetics
The term “antibiotic” includes a variety of chemical
compounds that exhibit great differences among them Pharmacokinetics is the study of the interrela-
in terms of mechanism of action and physicochemical, tionship between drug dose and variations in con-
pharmacokinetic, and pharmacodynamic characteris- centrations in plasma and tissue over time. The
tics. The uniqueness of each class makes independent most relevant pharmacokinetic parameters include
study essential to provide accurate characterization the following12:
of antibiotic behavior.
• peak concentration achieved after a single
dose (Cmax)
Physicochemistry • Vd: the apparent volume of fluid that contains
the total drug dose administered at the same
A simple, but useful chemical classification for concentration as in plasma
antibiotics is by their affinity for water. Hydrophilic • clearance (CL): quantification of the irrevers-
drugs predominantly distribute into intravascular ible loss of drug from the body by metabo-
and interstitial water but are unable to passively cross lism and excretion
the lipid cellular membrane and, therefore, do not • elimination half-life: time required for the
penetrate intracellularly in meaningful concentrations. plasma concentration to fall by one-half
Hence, their volume of distribution (Vd) is equiva- • protein binding: proportion of drug binding
to plasma proteins
Manuscript received September 13, 2010; revision accepted
January 3, 2011.
• AUC0-24: total area under the concentration
Affiliations: From the Burns, Trauma and Critical Care Research curve over 0 to 24 h
Centre (Drs Ulldemolins, Roberts, and Lipman), The University
of Queensland, Brisbane, QLD, Australia; Critical Care Depart-
ment (Drs Ulldemolins and Rello), Vall d’Hebron University
Hospital, Vall d’Hebron Institut de Recerca (VHIR), Universitat Pharmacodynamics and PK /PD
Autònoma de Barcelona, Barcelona, Spain; Centro de Investigación
Biomédica En Red de Enfermedades Respiratorias (CIBERES) Pharmacodynamics is the study of the relationship
(Drs Ulldemolins and Rello), Barcelona, Spain; and Department between drug concentrations and effect.12 The PK/PD
of Intensive Care Medicine (Drs Roberts and Lipman) and Phar- approach seeks to establish a relationship between
macy Department (Dr Roberts), Royal Brisbane and Women’s
Hospital, Herston, Brisbane, QLD, Australia. dosage and pharmacological effect.12 Figure 1 repre-
Funding/Support: Funded by the National Health and Medical sents the relationship among pharmacokinetics, phar-
Research Council of Australia [Project Grant 519702; Australian macodynamics, and PK/PD. Antibiotics can be cate-
Based Health Professional Research Fellowship 569917
(to Dr Roberts)]; Australia and New Zealand College of Anaes- gorized in three different classes depending on the
thetists [ANZCA 06/037 and 09/032]; Queensland Health-Health PK/PD indices associated with their optimal killing
Practitioner Research Scheme; Royal Brisbane and Women’s activity.13
Hospital Research Foundation (to Drs Roberts and Lipman); and
CIBERES [0606036], Agència de Gestió d’Ajuts Universitaris i de
Recerca [09/SGR/1226], and Fondo de Investigación Sanitaria Time-Dependent Antibiotics: Optimal activity is achieved
[07/90960] (to Drs Ulldemolins and Rello). when unbound plasma concentrations are maintained
Correspondence to: Jordi Rello, MD, PhD, Critical Care Depart- above the minimum inhibitory concentration (MIC)
ment, Vall d’Hebron University Hospital, Institut de Recerca
Vall d’Hebron-UAB, Passeig de la Vall d’Hebron 119-129, 08035 of the bacteria (ƒ T . MIC) for a defined fraction of
Barcelona, Spain; e-mail: jrello.hj23.ics@gencat.cat the dosing interval.
© 2011 American College of Chest Physicians. Reproduction
of this article is prohibited without written permission from the Concentration-Dependent Antibiotics: Optimal activity
American College of Chest Physicians (http://www.chestpubs.org/
site/misc/reprints.xhtml). correlates with Cmax, quantified by its ratio with the
DOI: 10.1378/chest.10-2371 MIC of the bacteria (Cmax/MIC).
www.chestpubs.org CHEST / 139 / 5 / MAY, 2011 1211
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
© 2011 American College of Chest Physicians
- 4. Figure 1. Interrelationship among pharmacokinetics, pharmacodynamics, and pharmacokinetics/
pharmacodynamics.
Concentration-Dependent Antibiotics With Time Later, typical features of septic shock may appear,
Dependence: A defined ratio between the unbound including a decrease in cardiac output and BP.17 This
AUC0-24 and the MIC of the bacteria (ƒAUC0-24/MIC) sepsis-mediated altered blood flow may have impor-
correlates with optimal activity. tant effects on drug delivery to tissues.
During the warm shock phase, hypoperfusion of
vital organs (eg, brain or lung) occurs, whereas
Pathophysiology of MODS and Effect peripheral tissues and nonvital organs still receive
on Drug Vd and CL high blood flow as a consequence of peripheral vaso-
dilation and increased cardiac work.17 Vital organs
Sepsis-related MODS has been defined as the hypoperfusion can lead to suboptimal delivery of
worsening of organ function due to a severe infection antibiotic and subtherapeutic levels at the target site
such that homeostasis cannot be maintained without during the initial stages of the infection in vital organ
intervention, usually involving two or more organ infections (eg, respiratory tract infections). However,
systems.14 Endotoxins have a cascade effect on the a challenge for interpretation is the absence of phar-
production of endogenous molecules that act on the macokinetic data specifically targeting the effects of
vascular endothelium, leading to vasodilatation and warm shock on drug distribution, and more research
transcapillary leakage of fluid and proteins into the is required in this area.
extracellular space.15 Moreover, sepsis is known to Peripheral tissue hypoperfusion can occur during
produce myocardial dysfunction.16 These hemody- the second phase of septic shock as a result of the body’s
namic alterations lead to sepsis-induced tissue hypop- attempt to increase perfusion of the vital organs.18
erfusion, which can affect pharmacokinetics. Because Because peripheral tissues frequently are the source
antibiotics are a group of drugs with “silent” pharma- of infection,19 hypoperfusion can lead to a failure to
codynamics (ie, the pharmacologic effect is not per- attain therapeutic concentrations at the site of infec-
ceivable immediately after administration), it is almost tion.20 A similar scenario may be observed in patients
impossible to assess whether therapeutic concentra- with fluid shifts, capillary leak, and edema.21 In this
tions are being achieved during the early phase of case, despite increased movement of plasma and
therapy. Therefore, consideration of the scenarios likely solutes (eg, hydrophilic antibiotics) to the extravas-
to alter antibiotic pharmacokinetics and necessitate cular compartment, drug concentrations at the tar-
dosage adjustment are necessary to enable individu- get site could decrease because of a dilution effect.21
alization of antibiotic therapy. Alternative approaches to drug administration, such
as continuous or extended infusion, have been shown
to reach more consistent antibiotic concentrations
Tissue Hypoperfusion
in tissue for time-dependent antibiotics in these
In the first stage of septic shock (warm shock), scenarios and should be considered when treating
arteries dilate, decreasing peripheral arterial resis- infections by poorly susceptible bacteria.22,23 Monte
tance and causing a reflex increase in cardiac output. Carlo simulations can be used to this end to compare
1212 Postgraduate Education Corner
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
© 2011 American College of Chest Physicians
- 5. the relative PK/PD target attainments for different related cachexia) and are rarely at steady state, these
dosing approaches for antibiotics, particularly for formulas may lead to inaccurate estimations of GFR
time-dependent antibiotics. These analyses have shown and lead to inappropriate dose adjustments.28,29 Where
consistently that extended infusions (. 3 h) or contin- possible, it is preferable to use either 8-, 12-, or
uous infusions of time-dependent antibiotics achieve 24-h urinary CrCL to estimate GFR in critically ill
PK/PD targets more successfully than intermittent patients.30-32
infusions (Յ 30 min).24-26 Monte Carlo simulations When using urinary CrCL, dose recommendations
also can be used to show the effect of renal dysfunc- in the product information for estimated GFR by
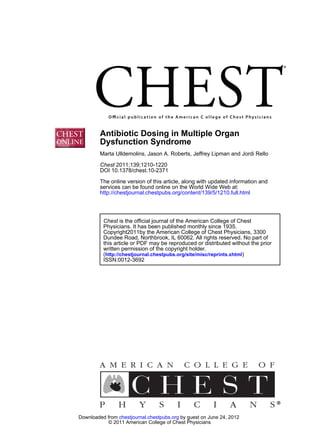
tion on the achievement of PK/PD targets. Figure 2 MDRD or Cockroft-Gault also apply. The main issue
has been adapted from Roberts et al22 and describes here is not the change in drug CL relative to GFR
how administering the same dose of meropenem in that is problematic; rather, it is how GFR is calcu-
different levels of renal dysfunction will provide dif- lated. If GFR is not accurately estimated, then any
ferent levels of achievement of PK/PD targets. Use of dose adjustment is likely to be suboptimal.
extended or continuous infusions in this context could
serve to further increase the achievement of PK/PD
Hepatic Dysfunction
targets.
The most common causes of liver failure in criti-
Renal Dysfunction cally ill patients are infection-related cholestasis and
hepatocellular injury, which occur in response to bac-
Several factors can precipitate acute kidney injury terial toxins and to the toxins themselves.33 In the first
(AKI) in critically ill patients.27 Early identification case, bacterial toxins and released cytokines can
of AKI and accurate assessment of renal function affect the uptake and excretion of bile by hepatocytes,
are essential for daily dose adjustment of hydrophilic leading to jaundice. In the second case, endotoxins
antibiotics. The estimations of creatinine clearance and bacteria are phagocytized by Kupffer cells that
(CrCL) as a surrogate for glomerular filtration rate release several hepatotoxic molecules, leading to cel-
(GFR) using formulas such as Cockroft-Gault and lular damage.33 Hepatic dysfunction also may result
modified diet in renal disease (MDRD) must be from organ hypoperfusion, hemolysis, or concomi-
interpreted carefully in critically ill patients because tant administration of hepatotoxic drugs (eg, rifam-
despite having well-documented clinical value in spe- picin).33,34 Assessment of the degree of hepatic dys-
cific patient populations (eg, patients with chronic kid- function in acute liver failure is mainly clinical and
ney disease), they are yet to be validated in critically may include signs and symptoms such as elevations in
ill patients. Because plasma creatinine concentrations liver enzymes, bilirubin, or ammonia and decreases in
can vary for many reasons other than renal function the concentration of liver-produced proteins (eg, albu-
in these patients (eg, decreases due to immobility- min, a1-acid glycoprotein, coagulation factors). Hepatic
dysfunction may impair metabolism and, therefore,
lead to accumulation of hepatically cleared antibi-
otics.35,36 A decrease in the hepatic production of
albumin and a1-acid glycoprotein also can alter phar-
macokinetics of highly protein-bound antibiotics.25,37,38
Albumin is the most frequent drug carrier in the
bloodstream. The drug-protein interaction is rapid
and dynamic, and an equilibrium depends on the
concentration of both drug and protein.39 In the
presence of hypoalbuminemia, a larger number of
unbound drug molecules are able to distribute from
the bloodstream into tissues to a larger extent than
when there is normal protein binding; pharmacoki-
netically, this is translated into a larger Vd.39
Figure 2. The effect of varying levels of renal dysfunction on Furthermore, clinical management of severe hepatic
the achievement of pharmacokinetics/pharmacodynamics targets failure may include renal replacement therapy (RRT)
for the same dose of meropenem. This example describes the prob- and the use of adsorbent columns for removing excess
ability of target attainment (fT . MIC) for meropenem administered
by intermittent bolus (infused over 5 min), in a man aged 50 years ammonia and other waste products in the blood.40
and weighing 70 kg with Cr of 50, 100, 200, and 300 mmol/L. The additive effect of these interventions and endog-
Cr 5 plasma creatinine concentration; f T . MIC 5 time over the enous renal function on the excretion of renally
minimum inhibitory concentration; MIC 5 minimum inhibitory
concentration. Adapted with permission of Oxford University Press cleared antibiotics has to be considered when dosing
from Roberts et al.22 with hydrophilic antibiotics.
www.chestpubs.org CHEST / 139 / 5 / MAY, 2011 1213
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
© 2011 American College of Chest Physicians
- 6. Optimizing Initial Dosing of Antibiotics therapeutic concentrations.49 This is the same prin-
in MODS ciple by which loading doses of drugs such as amio-
darone and phenytoin are required.50,51 Further,
Pharmacokinetic alterations mediated by MODS evidence supports that even the Vd of hydrophilic
should be considered during antibiotic prescription antibiotics is increased in obese patients due to
in critically ill patients. During the initial phase of the increased interstitial fluid, connective tissue, and
sepsis, increased Vd and CL are common, and dosing muscle mass also present in obesity.52,53 Therefore,
must be adjusted,11,41,42 which has been confirmed by obesity must be a factor to consider for initial dosing.
two recent studies. The first study, by Roberts et al,43 In this context, use of an equation that assists cal-
was a b-lactam therapeutic drug monitoring (TDM) culation of lean body weight should be used.54
evaluation in critically ill patients, including patients Table 1 provides broad recommendations for opti-
with MODS, that found that %07 فof patients did mizing initial dosing in patients with increased Vd.
not achieve appropriate antibiotic concentrations, Table 2 provides guidance for specific drugs in this
with requirement of 50.4% and 23.7% dose increases scenario.
and decreases, respectively, on the initial phase of
therapy. The second was a multicenter study by
Taccone et al44 that showed that conventional initial Optimizing Maintenance Dosing
dosing for many b-lactams frequently used in criti- of Antibiotics in MODS
cally ill patients was insufficient for achieving PK/PD Maintenance dosing must be guided by drug CL.
targets on the first day of therapy. In this study, only Depending on the organ systems impaired by MODS,
28% of the patients on ceftazidime, 16% on cefepime, the effect on antibiotic CL can vary widely. The most
and 44% on piperacillin/tazobactam achieved the relevant organ systems that may affect pharmacoki-
PK/PD targets on the first day of therapy. The authors netics (mainly renal and hepatic systems) will be con-
found that 40% of patients receiving piperacillin/ sidered individually.
tazobactam had plasma concentrations of less than Table 1 provides general principles for mainte-
four times MIC within 90 min after administration. nance dosing in renal failure, hepatic failure, and
The results of both studies are likely to be due to RRT. Table 2 provides guidance for specific drugs in
an increased Vd for these patients.15,45 It is important these scenarios. Figure 3 summarizes the scenarios
to note that in the study by Taccone et al,44 27% of the likely to alter pharmacokinetics in MODS.
patients had AKI, and despite having been prescribed
with standard non-AKI initial doses, most of them
had suboptimal concentrations after the first dose. Renal Dysfunction
In contrast, in the study by Roberts et al,43 19% of Hydrophilic antibiotics are mostly renally cleared by
patients had AKI (with or without dialysis require- glomerular filtration and tubular secretion. Decreased
ments), and on days 2 through 5, 72% of these patients CL of these drugs is well described in renal dysfunc-
required a dose decrease. The data from both studies tion, and as such, dose reductions or extended dosing
suggest that initial antibiotic dosing needs to account intervals are required to prevent drug accumulation
for the increased Vd that occurs in critically ill patients and toxicity.55 Dose adjustments to prevent toxicity
with MODS15; therefore, higher-than-standard doses are especially relevant for antibiotics with a narrow
should be considered in the initial phase of therapy. therapeutic window, such as glycopeptides and amin-
This concept will be referred throughout this review oglycosides, that can produce nephrotoxicity, and,
as “front-loaded” dosing and especially applies to hence, its accumulation may lead to a vicious circle of
hydrophilic drugs whose Vd dramatically increases in injury in the damaged kidney that may lead to greater
this scenario.22,23,46,47 This concept was demonstrated antibiotic accumulation.
by Marik46 who showed a twofold increase in the When dose reducing, it is essential to consider anti-
Vd of amikacin in critically ill patients with gram- biotic pharmacodynamics to ensure that targets are
negative infections. This pharmacokinetic alteration will still attained where possible. For instance, a more appro-
significantly affect the achievement of therapeutic priate dose reduction of time-dependent antibiotics
peak concentrations (Cmax/MIC Ն 10).46 Recent would be to reduce the dose rather than the fre-
research also supports administration of front-loaded quency of administration as a strategy to preserve the
doses for aminoglycosides (eg, 25 mg/kg for amikacin) ƒ T . MIC (eg, recommended dosing of meropenem
on the first day of therapy for severe sepsis and septic for an estimated GFR , 15 mL/min would be a front-
shock.48 loaded dose of 1,000 mg to provide therapeutic con-
For lipophilic drugs, front-loaded doses based on centrations followed by a maintenance dose of 500 mg
total body weight should be considered for patients every 12 h to enable continued optimization of ƒ T . MIC
with a higher proportion of adipose tissue to achieve without toxicity). For concentration-dependent drugs,
1214 Postgraduate Education Corner
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
© 2011 American College of Chest Physicians
- 7. www.chestpubs.org
Table 1—Broad Guidelines for Loading and Maintenance Dosing of Antibiotics in Critically Ill Patients With MODS
Main Organ Systems PD Parameter Associated LD in Patients With
Antibiotic Solubility Responsible for Clearance With Maximal Activity Increased Vd MD in Acute Kidney Injury MD in Hepatic Failure
b-Lactams Hydrophilic Renal ƒ T . MIC Administer a high LD on Dose decreases preferred Normal dosing
day 1, as Vd will be to increased time between
significantly increased intervals
Aminoglycosides Hydrophilic Renal Cmax/MIC Administer a high LD on Increased time intervals Normal dosing
day 1, as Vd will be preferred to dose decreases,
significantly increased titrate dosing according
to TDM results
Glycopeptides Hydrophilic Renal AUC0-24/MIC Administer high LD on Titrate dosing according Normal dosing
day 1, as Vd will be to TDM results
significantly increased
Fluoroquinolones Lipophilic Renal and hepatic AUC0-24/MIC and Administer dosing for Decrease dose based on the Decrease dose based on the
(ciprofloxacin, Cmax/MIC conserved organ degree of organ dysfunction degree of organ dysfunction
moxifloxacin), renal function on day 1 and principal organ system and principal organ system
(levofloxacin) responsible for clearance responsible for clearance
Lincosamides Lipophilic Renal and hepatic AUC0-24/MIC and Administer dosing for Decrease dose based on Decrease dose based on the
ƒ T . MIC conserved organ the degree of organ degree of organ dysfunction
function on day 1 dysfunction
Macrolides Lipophilic Hepatic ƒ T . MIC and Normal dosing Normal dosing Normal dosing
AUC0-24/MIC
Nitroimidazoles Lipophilic Hepatic Cmax/MIC Normal dosing Normal dosing Decrease dosing if severe
(metronidazole) hepatic failure
Cyclic lipopeptides Amphiphilic Renal Cmax/MIC Administer a high LD on Increase dosing interval Normal dosing
© 2011 American College of Chest Physicians
(lipophilic and day 1, as Vd will be
hydrophilic) significantly increased
Glycylcyclines Lipophilic Hepatic AUC0-24/MIC Administer LD per Normal dosing Decrease dosing
product information
Oxazolidinones Lipophilic Hepatic AUC0-24/MIC and Normal dosing Normal dosing Normal dosing
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
ƒ T . MIC
AUC0-24/MIC 5 area under the concentration curve over 0 to 24 h-to-minimum inhibitory concentration ratio; Cmax/MIC 5 peak concentration-to-minimum inhibitory concentration ratio; ƒT . MIC 5 time over
the minimum inhibitory concentration; LD 5 front-loaded dose; MD 5 maintenance dose; MIC 5 minimum inhibitory concentration; MODS 5 multiple organ dysfunction syndrome; PD5pharmacodynamic;
TDM 5 therapeutic drug monitoring; Vd 5 volume of distribution.
CHEST / 139 / 5 / MAY, 2011
1215
- 8. Table 2—Dose Recommendations for LD and MD in MODS by Individual Drugs
1216
Recommended LD for Recommended MD for Recommended MD for Recommended MD for
Antibiotic Class Antibiotic Name Patients With -Vd (Day 1) Patients With Hepatic Failurea Patients With Acute Kidney Injurya Patients With RRTb
b-Lactams
Carbapenems Meropenem 1-2 g q8h 1 g q8h 500 mg q12h 500 mg q8h
Ertapenem 1 g q12h 1 g q12h 500 mg q12h 500 mg q8-12h
Penicillins Piperacillin/tazobactam 4.5 g q4-6h 4.5 g q6h 4.5 g q8h or 2.25 g q6h 4.5 g q8h
Ticarcillin/clavulanate 3.1 g q4-6h 3.1 g q6h 2 g q4-6h 2 g q4-6h
Isoxazolyl penicillins 2 g q4h 2 g q4h 2 g q6h-1g q4h 2 g q6h-1g q4h
(cloxacillin,
flucloxacillin,
dicloxacillin)
Cephalosporins Ceftriaxone 1-2 g q12h 1 g q12h 1 g q12h 1-2g q12h
Ceftazidime 2 g q8h 2 g q8h 1 g q8h 1 g q8h
Cefepime 1-2 g q8-12h 1-2 g q8-12h 500 mg-1 g q12h 1-2 g q12h
Monobactams Aztreonam 1-2 g q8h 1 g q6-8h 500 mg q6-8h 500 mg q6-8h
Aminoglycosides Amikacin 25 mg/kg q24h to achieve 15 mg/kg q24h; monitor Monitor Cmin after 24 h, aiming Monitor Cmin after 24 h,
a Cmax/MIC 5 10 Cmin after 24 h, aiming for levels , 5 mg/L. Dosing aiming for levels , 5 mg/L
for levels , 5 mg/L q48h may be required for and titrate dosing according
severe renal dysfunction to results
Gentamycin, 7 mg/kg as a LD on day 1 to 5 mg/kg q24h; monitor Monitor Cmin after 24 h, aiming Monitor Cmin after 24 h,
tobramycin achieve a Cmax/MIC 5 10 Cmin after 24 h, aiming for levels , 0.5 mg/L. Dosing aiming for levels , 0.5 mg/L
for levels , 0.5 mg/L q48h may be required for and titrate dosing according
severe renal dysfunction to results
Glycopeptides Vancomycin 20-30 mg/kg LDc 15-20 mg/kg q12h Use TDM (Cmin) on day 3, Use TDM (Cmin) on day 3,
aiming for range 15-20 mg/L aiming for range 15-20 mg/L
(20-25 mg/L if CI). Dosing (20-25 mg/L if CI). Dosing
must be titrated to fit in this range should be titrated to this
range
Teicoplanin 12 mg/kg q12h for 3-6 mg/kg q12h, titrate Prescribe 3 mg/kg q12h from the Prescribe 3 mg/kg q12h from the
© 2011 American College of Chest Physicians
three doses dosing on day 4 guided fourth dose and titrate dosing fourth dose and titrate dosing
by TDM, aiming for on day 4 guided by TDM, aiming on day 4 guided by TDM,
Cmin . 10 mg/L for Cmin . 10 mg/L aiming for Cmin . 10 mg/L
Fluoroquinolones Ciprofloxacin 400 mg q8h 400 mg q12-24h 400 mg q12-24h 400 mg q12-24h
Levofloxacin 500-750 mg q24h 500-750 mg q24h 250 mg q24-48h 500 mg q48h or 250 mg q24h
Moxifloxacin 400 mg q24h 400 mg q24h 400 mg q24h 400 mg q24h
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
Lincosamides Lincomycin Administer 600 mg q6-8h 600 mg q12h 600 mg q12h 600 mg q8h
as an LD on day 1
Clindamycin Administer 600 mg q6-8h 600 mg q12-24h 600 mg q8h 600 mg q8h
as an LD on day 1
Macrolides Clarithromycin 500 mg q12h 500 mg q12h In severe renal failure, 500 mg q12h
250 mg q12h
Azithromycin 500 mg q24h 500 mg q24h 500 mg q24h 500 mg q24h
(Continued)
Postgraduate Education Corner
- 9. Data are modified from the product information of each particular drug. Note that the product information for many of the hydrophilic antibiotics included in the table (except teicoplanin and the amino-
glycosides) does not consider different dosing schedules for LDs and MDs and is based on studies of patients who were not critically ill. The recommended LDs are based on data from critically ill patients
like aminoglycosides, it is suggested to prolong the
interval between doses rather than to decrease the
Recommended MD for
Patients With RRTb
dose so that the peak concentration required for opti-
12 h after LD, administer
mal bacterial killing is still achieved.11
However, despite these theoretical recommenda-
50-100 mg q12h
tions, uncertainty is always present when prescribing
6 mg/kg q48h
600 mg q12h
500 mg q8h
antibiotics in patients with MODS because organ
to enable rapid attainment of therapeutic concentrations. Cmin 5 trough concentration; RRT 5 renal replacement therapy. See Table 1 legend for expansion of other abbreviations.
function is very likely to fluctuate from day to day during
therapy. It follows that TDM is a very useful tool to
titrate antibiotic dosing in MODS. TDM is widely used
with aminoglycosides and glycopeptides to ensure
appropriate exposure and minimize the incidence of
Patients With Acute Kidney Injurya
toxicity.56 However, the potential and usefulness of
Recommended MD for
TDM as a strategy for optimizing antibiotic doses of
b-lactams (the most frequently prescribed class of anti-
12 h after LD, administer
biotics) has not yet been confirmed. Recent research
50-100 mg q12h
has assessed its usefulness with a broad group of criti-
cally ill patients.43,44 Roberts et al43 showed that in the
6 mg/kg q48h
600 mg q12h
500 mg q8h
maintenance phase of therapy, many patients with renal
dysfunction required a dose decrease due to high con-
cThere are few data measuring toxicity of vancomycin LDs; therefore, we would suggest not administering LDs that exceed 35 mg/kg.
centrations (about 10 times MIC), despite empirical
dose adjustment for renal dysfunction. However, some
other patients with renal failure or on RRT exhibit sub-
Patients With Hepatic Failurea
optimal concentrations with this adjusted dosing, which
500 mg q12-24h in severe
12 h after LD, administer
Recommended MD for
evidences that concentrations do not depend exclusively
Table 2—Continued
on renal function but on various other factors.
hepatic failure
25 mg q12h
6 mg/kg q24h
600 mg q12h
Renal Replacement Therapy
As renal function deteriorates, waste products will
accumulate, and commencement of RRT should be
considered. The main determinants of CL during RRT
are the modality and settings prescribed. Hemodial-
ysis, hemofiltration, hemodiafiltration, and peritoneal
Patients With -Vd (Day 1)
Recommended LD for
dialysis all have different mechanisms of removing
aActual dose prescribed will be guided by the actual level of organ dysfunction.
metabolic waste and have a different effect on the
extent to which each drug is cleared. Other factors
6-8 mg/kg q24h
600 mg q8-12h
100 mg dose 1
that determine the extraction ratio are drug molec-
500 mg q8h
ular weight (drugs with a molecular weight greater
than the pores of the filter membrane are not able to
be removed), protein binding (only unbound mole-
cules can be removed), drug affinity for filter adsorp-
bDose depends on data available for dialysis settings.
tion, whether replacement fluid is added prefilter or
postfilter, and the ultrafiltration rate.57 The implica-
Antibiotic Name
tions of RRT on drug dosing have been reviewed
Metronidazole
recently,57 and a further discussion is beyond the
Daptomycin
Tigecycline
scope of this article. However, Table 1 provides some
Linezolid
recommendations for dosing in RRT.
Hepatic Dysfunction
Cyclic lipopeptides
Liver impairment may have a significant impact on
Nitroimidazoles
Antibiotic Class
Oxazolidinones
Glycylcyclines
the CL of both lipophilic and hydrophilic drugs.
Lipophilic drugs may undergo metabolism in the
liver to increase the hydrophilicity of the compound.
The CL of hepatically eliminated drugs depends on
www.chestpubs.org CHEST / 139 / 5 / MAY, 2011 1217
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
© 2011 American College of Chest Physicians
- 10. Figure 3. Clinical scenarios likely to alter antibiotic PK in MODS. MODS 5 multiple organ dysfunction
syndrome; PK 5 pharmacokinetics.
the hepatic blood flow and intrinsic clearance (ie, otics (Table 2) account for this scenario. Maintenance
degree of enzymatic activity). Therefore, two kinds of dosing should be guided by the level of organ func-
scenarios can be distinguished. CL of highly extracted tion and in the context of the main elimination path-
drugs is mainly correlated with hepatic blood flow ways for the drug and, where possible, guided by
(eg, lidocaine), whereas in less-extracted drugs, CL TDM. Decreased plasma concentrations of a1-acid
is determined by intrinsic CL and degree of pro- glycoprotein increase substantially erythromycin Vd
tein binding (eg, nitroimidazoles, fluoroquinolones).12 (73%-81% protein bound), whereas CL decreases
Hepatic failure may imply modification of both fac- by 60% in the presence of metabolic impairment.62
tors, leading to decreased drug elimination, accumu- Other antibiotics that bind substantially to this protein
lation, and potential toxicity. For example, in liver include trimethoprim and the lincosamides.63
failure, metronidazole oxidation by microsomes may As a final consideration for organ dysfunction, it is
be decreased because of reduced enzyme expression noteworthy that critically ill patients can present with
and enzymatic activity,58 leading to potential toxic- underlying comorbidities, such as chronic renal or
ities, including seizures and peripheral neuropathy. hepatic dysfunction, unrelated to sepsis. In this case,
Other drugs may be cleared by biliary excretion, the previously mentioned dosing principles for initial
which may be substantially decreased in hepatic and maintenance dosing also should apply. Dose
impairment (eg, tigecycline). A study comparing adjustments should always be made according to the
patients with different degrees of hepatic failure degree of organ function and the estimated level of
found that tigecycline CL was reduced by 55%, and drug Vd and CL present in the patient, regardless of
elimination half-life was prolonged by 43% in patients preexisting dysfunction. Preexisting dysfunction should
with severe hepatic impairment. In this context, a only be considered as a guide to the likely level of
dose reduction is suggested to avoid toxicity.59 organ function in the maintenance phase of therapy.
Additionally, the decreased synthesis of albumin and
a1-acid glycoprotein in liver dysfunction, together with
the transcapillary distribution of these proteins due Conclusions
to capillary leakage,60 may alter the pharmacokinetics
of highly protein-bound antibiotics. Hypoalbuminemia Appropriate antibiotic dosing in MODS is complex
has been shown to cause significant increases in the and depends on several drug- and patient-related fac-
Vd and CL of drugs such as ceftriaxone (85%-95% tors. Consideration of antibiotic physicochemical and
protein bound), ertapenem (85%-95%), flucloxacillin pharmacodynamic characteristics and disease-related
(95%), and teicoplanin (90%-95%).25,37,38,61 Therefore, alterations in pharmacokinetics is essential for design-
front-loaded doses should be considered when pre- ing dosing regimens that avoid suboptimal dosing.
scribing these drugs in critically ill patients with There are two important phases in antibiotic therapy
MODS and hypoalbuminemia.39 Initial dosing rec- in MODS. During the first day of therapy, front-
ommendations for highly bound hydrophilic antibi- loaded dosing is required and must be guided by the
1218 Postgraduate Education Corner
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
© 2011 American College of Chest Physicians
- 11. predicted Vd, which is likely to be increased in critically terns in empiric antibiotic therapy for HAP/VAP [published
ill patients despite impaired organ function. From online ahead of print September 16, 2010]. Eur Respir J.
doi:10.1183/09031936.00093010.
day 2 onward, maintenance dosing can be adjusted in 11. Roberts JA, Lipman J. Pharmacokinetic issues for antibi-
line with the CL associated with the organ dysfunc- otics in the critically ill patient. Crit Care Med. 2009;37(3):
tion. The requirements for dose adjustment for anti- 840-851.
biotics should be considered individually depending 12. Rowland M, Tozer TN. Clinical Pharmacokinetics: Concepts
on the organ system that is failing and the drug and Applications. 3rd ed. Philadelphia, PA: Lippincott
Williams & Wilkins; 1995.
CL pathway. Because of the great variability of organ 13. Craig WA. Pharmacokinetic/pharmacodynamic parameters:
function during a septic insult, TDM should be rationale for antibacterial dosing of mice and men. Clin Infect
regarded as a useful tool to individualize dosing and Dis. 1998;26(1):1-10.
ensure appropriate exposure to the antibiotic. Further 14. American College of Chest Physicians/Society of Critical Care
research on dose adjustment in MODS is required Medicine Consensus Conference: definitions for sepsis and
organ failure and guidelines for the use of innovative ther-
for improving patient quality of care and outcomes in apies in sepsis. Crit Care Med. 1992;20(6):864-874.
this population. 15. van der Poll T. Immunotherapy of sepsis. Lancet Infect Dis.
2001;1(3):165-174.
16. Thijs LG, Schneider AJ, Groeneveld AB. The haemodynam-
Acknowledgments ics of septic shock. Intensive Care Med. 1990;16(suppl 3):
Financial/nonfinancial disclosures: The authors have reported S182-S186.
to CHEST the following conflicts of interest: Dr Roberts serves 17. The Merck Manuals Online Medical Library. Merck and Co, Inc
as a consultant for AstraZeneca and Janssen-Cilag. Dr Lipman Web site. http://www.merckmanuals.com/professional/index.
serves as a consultant for AstraZeneca and Wyeth and has received html. Accessed November 2010.
grant support from AstraZeneca. Drs Ulldemolins and Rello have 18. Jones AE, Puskarich MA. Sepsis-induced tissue hypoperfu-
reported that no potential conflicts of interest exist with any com- sion. Crit Care Clin. 2009;25(4):769-779.
panies/organizations whose products or services may be discussed
in this article. 19. Ryan DM. Pharmacokinetics of antibiotics in natural and exper-
imental superficial compartments in animals and humans.
J Antimicrob Chemother. 1993;31(suppl D):1-16.
20. Joukhadar C, Frossard M, Mayer BX, et al. Impaired tar-
References get site penetration of beta-lactams may account for ther-
1. Spellberg B, Guidos R, Gilbert D, et al; Infectious Diseases apeutic failure in patients with septic shock. Crit Care Med.
Society of America. The epidemic of antibiotic-resistant infec- 2001;29(2):385-391.
tions: a call to action for the medical community from the 21. Fleck A, Raines G, Hawker F, et al. Increased vascular per-
Infectious Diseases Society of America. Clin Infect Dis. 2008; meability: a major cause of hypoalbuminaemia in disease and
46(2):155-164. injury. Lancet. 1985;1(8432):781-784.
2. Pharmaceutical Research and Manufactures of America. 22. Roberts JA, Kirkpatrick CM, Roberts MS, Robertson TA,
Medicines in development. Pharmaceutical Research and Man- Dalley AJ, Lipman J. Meropenem dosing in critically ill
ufacturers of America Web site. http://www.phrma.org/new patients with sepsis and without renal dysfunction: intermit-
medicines. Accessed March 2010. tent bolus versus continuous administration? Monte Carlo
3. Roberts JA, Kruger P, Paterson DL, Lipman J. Antibiotic dosing simulations and subcutaneous tissue distribution.
resistance—what’s dosing got to do with it? Crit Care Med. J Antimicrob Chemother. 2009;64(1):142-150.
2008;36(8):2433-2440. 23. Roberts JA, Roberts MS, Robertson TA, Dalley AJ, Lipman J.
4. Kumar A, Ellis P, Arabi Y, et al; Cooperative Antimicrobial Piperacillin penetration into tissue of critically ill patients with
Therapy of Septic Shock Database Research Group. Ini- sepsis—bolus versus continuous administration? Crit Care Med.
tiation of inappropriate antimicrobial therapy results in a 2009;37(3):926-933.
fivefold reduction of survival in human septic shock. Chest. 24. Roberts JA, Kirkpatrick CM, Roberts MS, Dalley AJ, Lipman J.
2009;136(5):1237-1248. First-dose and steady-state population pharmacokinetics
5. Rello J, Gallego M, Mariscal D, Soñora R, Valles J. The value and pharmacodynamics of piperacillin by continuous or inter-
of routine microbial investigation in ventilator-associated pneu- mittent dosing in critically ill patients with sepsis. Int J
monia. Am J Respir Crit Care Med. 1997;156(1):196-200. Antimicrob Agents. 2010;35(2):156-163.
6. Garnacho-Montero J, Ortiz-Leyba C, Herrera-Melero I, et al. 25. Ulldemolins M, Roberts JA, Wallis SC, Rello J, Lipman J.
Mortality and morbidity attributable to inadequate empirical Flucloxacillin dosing in critically ill patients with hypoalbu-
antimicrobial therapy in patients admitted to the ICU with minaemia: special emphasis on unbound pharmacokinetics.
sepsis: a matched cohort study. J Antimicrob Chemother. J Antimicrob Chemother. 2010;65(8):1771-1778.
2008;61(2):436-441. 26. Roberts JA, Kwa A, Montakantikul P, Gomersall C, Kuti JL,
7. Paterson DL, Ko WC, Von Gottberg A, et al. Antibiotic Nicolau DP. Pharmacodynamic profiling of intravenous anti-
therapy for Klebsiella pneumoniae bacteremia: implications biotics against prevalent gram-negative organisms across
of production of extended-spectrum beta-lactamases. Clin the globe: the PASSPORT Program-Asia-Pacific Region.
Infect Dis. 2004;39(1):31-37. Int J Antimicrob Agents. 2011;37(3):225-229.
8. Lu CH, Chang WN, Chang HW. Klebsiella meningitis in 27. Ronco C, Bellomo R, Kellum J. Critical Care Nephrology.
adults: clinical features, prognostic factors and therapeutic 2nd ed. Philadelphia, PA: Saunders Elsevier; 2009;67-100,
outcomes. J Clin Neurosci. 2002;9(5):533-538. 157-196.
9. Ulldemolins M, Nuvials X, Palomar M, Masclans JR, Rello J. 28. Cockroft D, Gault M. Prediction of creatinine clearance from
Appropriateness is critical. Crit Care Clin. 2010;27(1):35-51. serum creatinine. Nephron. 1976;16(1):31-41.
10. Rello J, Ulldemolins M, Lisboa T, et al; the EU-VAP/CAP 29. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D;
Study Group. Determinants of choice and prescription pat- Modification of Diet in Renal Disease Study Group. A more
www.chestpubs.org CHEST / 139 / 5 / MAY, 2011 1219
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
© 2011 American College of Chest Physicians
- 12. accurate method to estimate glomerular filtration rate from spective study emphasizing the importance of a loading dose.
serum creatinine: a new prediction equation. Ann Intern Med. J Antimicrob Chemother. 2003;51(4):971-975.
1999;130(6):461-470. 48. Taccone FS, Laterre PF, Spapen H, et al. Revisiting the
30. Pong S, Seto W, Abdolell M, et al. 12-hour versus 24-hour loading dose of amikacin for patients with severe sepsis and
creatinine clearance in critically ill pediatric patients. septic shock. Crit Care. 2010;14(2):R53.
Pediatr Res. 2005;58(1):83-88. 49. Allard S, Kinzig M, Boivin G, Sörgel F, LeBel M. Intravenous
31. Wells M, Lipman J. Measurements of glomerular filtration in ciprofloxacin disposition in obesity. Clin Pharmacol Ther. 1993;
the intensive care unit are only a rough guide to renal func- 54(4):368-373.
tion. S Afr J Surg. 1997;35(1):20-23. 50. Chow MS. Intravenous amiodarone: pharmacology, pharma-
32. Wells M, Lipman J. Pitfalls in the prediction of renal func- cokinetics, and clinical use. Ann Pharmacother. 1996;30(6):
tion in the intensive care unit. A review. S Afr J Surg. 1997; 637-643.
35(1):16-19. 51. Richens A. Clinical pharmacokinetics of phenytoin.
33. Chand N, Sanyal AJ. Sepsis-induced cholestasis. Hepatology. Clin Pharmacokinet. 1979;4(3):153-169.
2007;45(1):230-241. 52. Bauer LA, Edwards WA, Dellinger EP, Simonowitz DA.
34. Marshall JC. Inflammation, coagulopathy, and the pathogen- Influence of weight on aminoglycoside pharmacokinetics
esis of multiple organ dysfunction syndrome. Crit Care Med. in normal weight and morbidly obese patients. Eur J Clin
2001;29(7 suppl):S99-S106. Pharmacol. 1983;24(5):643-647.
35. Greenfield RA, Gerber AU, Craig WA. Pharmacokinetics of 53. Blouin RA, Bauer LA, Miller DD, Record KE, Griffen WO Jr.
cefoperazone in patients with normal and impaired hepatic Vancomycin pharmacokinetics in normal and morbidly obese
and renal function. Rev Infect Dis. 1983;5(suppl 1):S127-S136. subjects. Antimicrob Agents Chemother. 1982;21(4):575-580.
36. Westphal JF, Brogard JM. Clinical pharmacokinetics of newer 54. Janmahasatian S, Duffull SB, Ash S, Ward LC, Byrne NM,
antibacterial agents in liver disease. Clin Pharmacokinet. Green B. Quantification of lean bodyweight. Clin Pharmacokinet.
1993;24(1):46-58. 2005;44(10):1051-1065.
37. Joynt GM, Lipman J, Gomersall CD, Young RJ, Wong EL, 55. Gilbert B, Robbins P, Livornese LL Jr. Use of antibacterial
Gin T. The pharmacokinetics of once-daily dosing of cef- agents in renal failure. Infect Dis Clin North Am. 2009;23(4):
triaxone in critically ill patients. J Antimicrob Chemother. 899-924.
2001;47(4):421-429. 56. Reed RL II, Wu AH, Miller-Crotchett P, Crotchett J, Fischer RP.
38. Burkhardt O, Kumar V, Katterwe D, et al. Ertapenem in Pharmacokinetic monitoring of nephrotoxic antibiotics in sur-
critically ill patients with early-onset ventilator-associated pneu- gical intensive care patients. J Trauma. 1989;29(11):1462-1468.
monia: pharmacokinetics with special consideration of free-drug discussion 1468-1470.
concentration. J Antimicrob Chemother. 2007;59(2):277-284. 57. Choi G, Gomersall CD, Tian Q, Joynt GM, Freebairn R,
39. Ulldemolins M, Roberts JA, Rello J, Paterson DL, Lipman J. Lipman J. Principles of antibacterial dosing in continuous
The effects of hypoalbuminemia on optimizing antibiotic dosing renal replacement therapy. Crit Care Med. 2009;37(7):
in critically ill patients. Clin Pharmacokinet. 2011;50(2):99-110. 2268-2282.
40. Hughes RD, Williams R. Use of sorbent columns and hae- 58. Farrell G, Baird-Lambert J, Cvejic M, Buchanan N. Dispo-
mofiltration in fulminant hepatic failure. Blood Purif. 1993; sition and metabolism of metronidazole in patients with liver
11(3):163-169. failure. Hepatology. 1984;4(4):722-726.
41. Roberts JA, Lipman J. Antibacterial dosing in intensive care: 59. Pfizer Pharmaceuticals. Tygacil1 (tigecycline) for injection: prod-
pharmacokinetics, degree of disease and pharmacodynamics uct information. Pfizer Web site. http://www.pfizerpro.com/
of sepsis. Clin Pharmacokinet. 2006;45(8):755-773. content/showlabeling.asp?id=491. Accessed January 2011.
42. Fuster-Lluch O , Gerónimo-Pardo M, Peyró-García R, 60. Rothschild MA, Oratz M, Zimmon D, Schreiber SS, Weiner I,
Lizán-García M. Glomerular hyperfiltration and albuminuria in Van Caneghem A. Albumin synthesis in cirrhotic subjects
critically ill patients. Anaesth Intensive Care. 2008;36(5):674-680. with ascites studied with carbonate-14C. J Clin Invest. 1969;
43. Roberts JA, Ulldemolins M, Roberts MS, et al. Therapeutic 48(2):344-350.
drug monitoring of beta-lactams in critically ill patients: proof 61. Barbot A, Venisse N, Rayeh F, Bouquet S, Debaene B,
of concept. Int J Antimicrob Agents. 2010;36(4):332-339. Mimoz O. Pharmacokinetics and pharmacodynamics of
44. Taccone FS, Laterre PF, Dugernier T, et al. Insufficient sequential intravenous and subcutaneous teicoplanin in crit-
b-lactam concentrations in the early phase of severe sepsis ically ill patients without vasopressors. Intensive Care Med.
and septic shock. Crit Care. 2010;14(4):R126. 2003;29(9):1528-1534.
45. Plank LD, Hill GL. Similarity of changes in body composi- 62. Barre J, Mallat A, Rosenbaum J, et al. Pharmacokinetics of
tion in intensive care patients following severe sepsis or major erythromycin in patients with severe cirrhosis. Respective
blunt injury. Ann N Y Acad Sci. 2000;904:592-602. influence of decreased serum binding and impaired liver
46. Marik PE. Aminoglycoside volume of distribution and illness metabolic capacity. Br J Clin Pharmacol. 1987;23(6):753-757.
severity in critically ill septic patients. Anaesth Intensive Care. 63. Son DS, Hariya S, Shimoda M, Kokue E. Contribution of
1993;21(2):172-173. alpha 1-acid glycoprotein to plasma protein binding of some
47. Pea F, Brollo L, Viale P, Pavan F, Furlanut M. Teicoplanin basic antimicrobials in pigs. J Vet Pharmacol Ther. 1996;
therapeutic drug monitoring in critically ill patients: a retro- 19(3):176-183.
1220 Postgraduate Education Corner
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
© 2011 American College of Chest Physicians
- 13. Antibiotic Dosing in Multiple Organ Dysfunction Syndrome
Marta Ulldemolins, Jason A. Roberts, Jeffrey Lipman and Jordi Rello
Chest 2011;139; 1210-1220
DOI 10.1378/chest.10-2371
This information is current as of June 24, 2012
Updated Information & Services
Updated Information and services can be found at:
http://chestjournal.chestpubs.org/content/139/5/1210.full.html
References
This article cites 61 articles, 18 of which can be accessed free at:
http://chestjournal.chestpubs.org/content/139/5/1210.full.html#ref-list-1
Cited Bys
This article has been cited by 2 HighWire-hosted articles:
http://chestjournal.chestpubs.org/content/139/5/1210.full.html#related-urls
Permissions & Licensing
Information about reproducing this article in parts (figures, tables) or in its entirety can be
found online at:
http://www.chestpubs.org/site/misc/reprints.xhtml
Reprints
Information about ordering reprints can be found online:
http://www.chestpubs.org/site/misc/reprints.xhtml
Citation Alerts
Receive free e-mail alerts when new articles cite this article. To sign up, select the
"Services" link to the right of the online article.
Images in PowerPoint format
Figures that appear in CHEST articles can be downloaded for teaching purposes in
PowerPoint slide format. See any online figure for directions.
Downloaded from chestjournal.chestpubs.org by guest on June 24, 2012
© 2011 American College of Chest Physicians