Downloaded 79 times
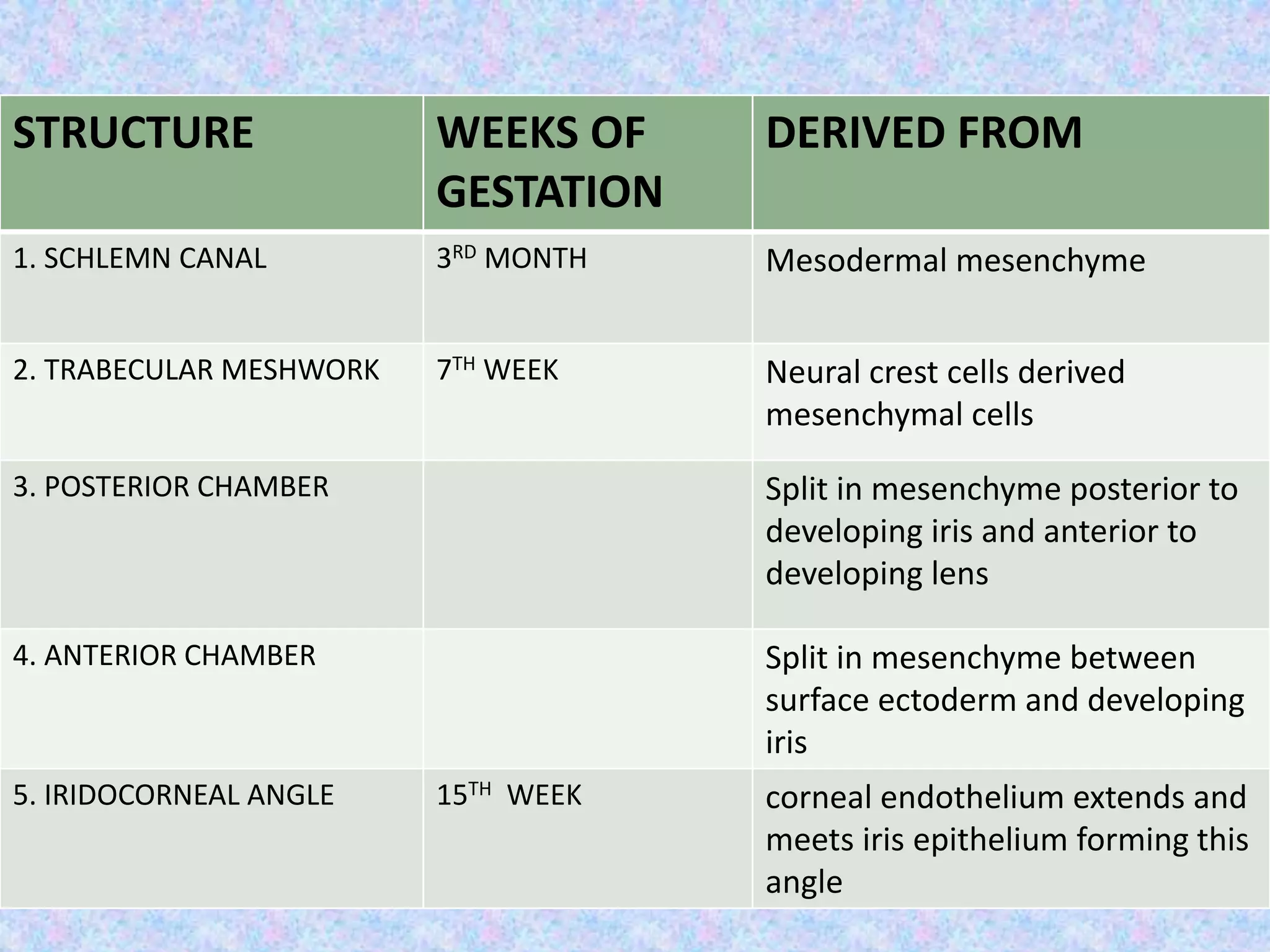
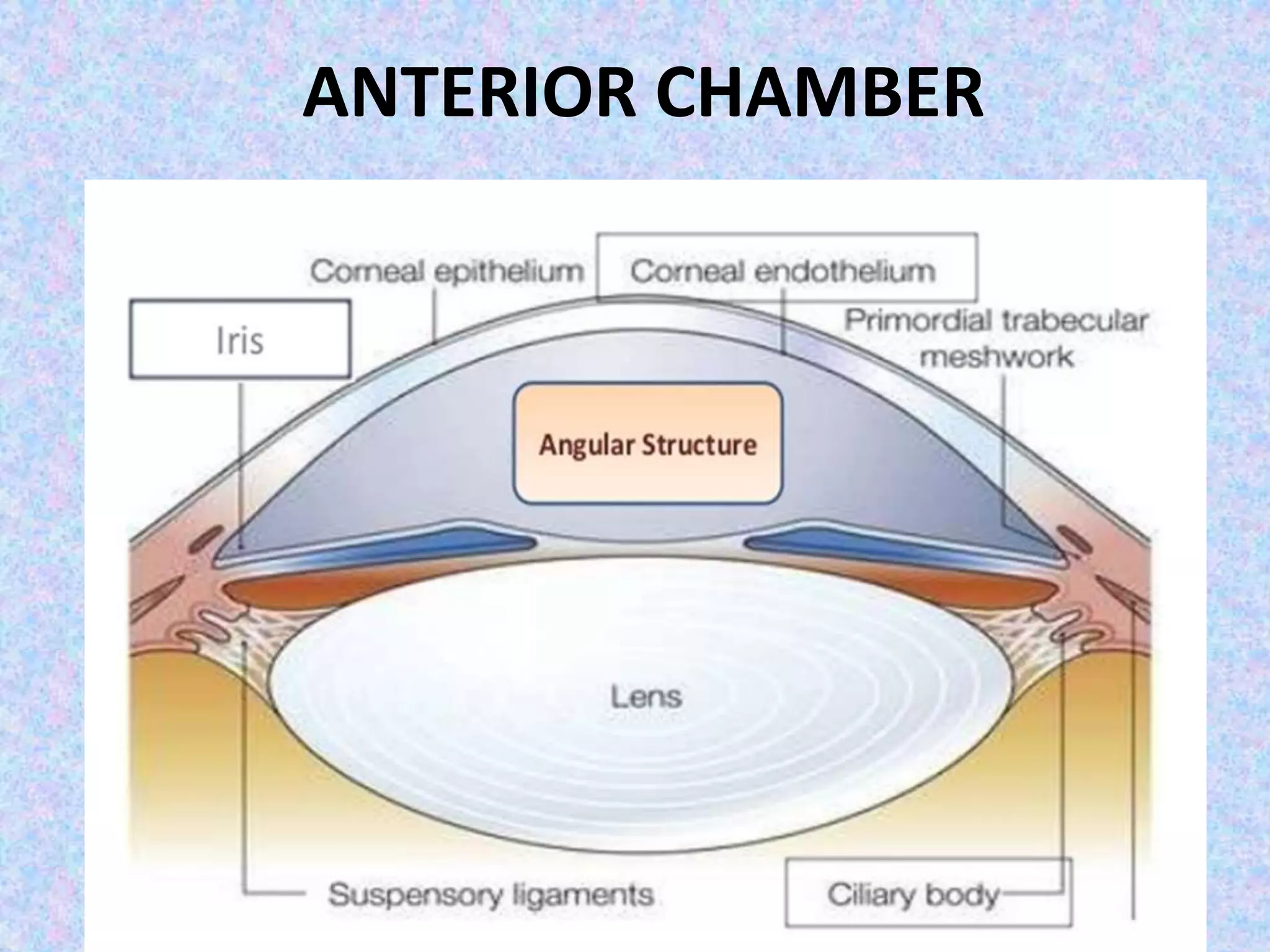
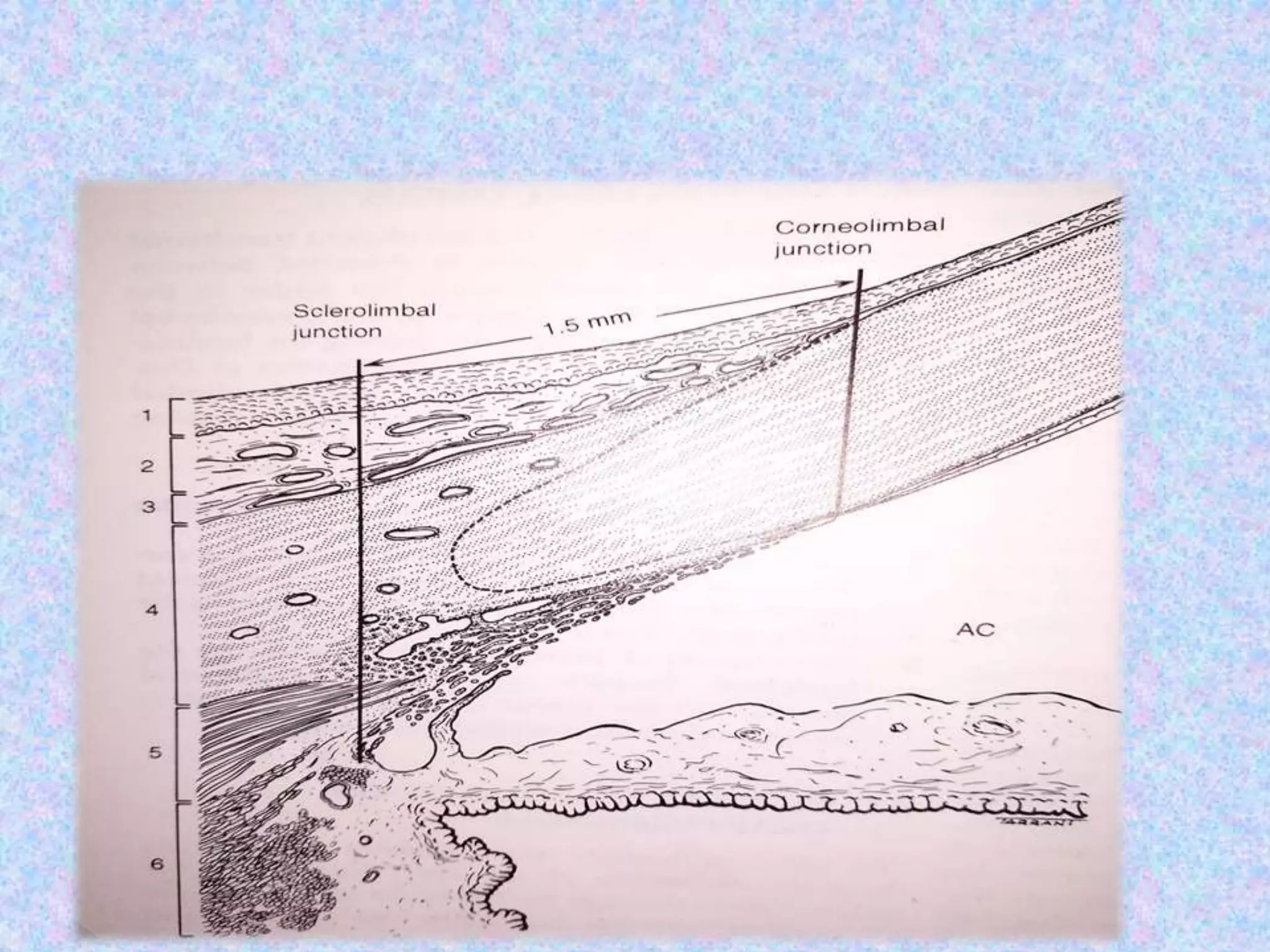
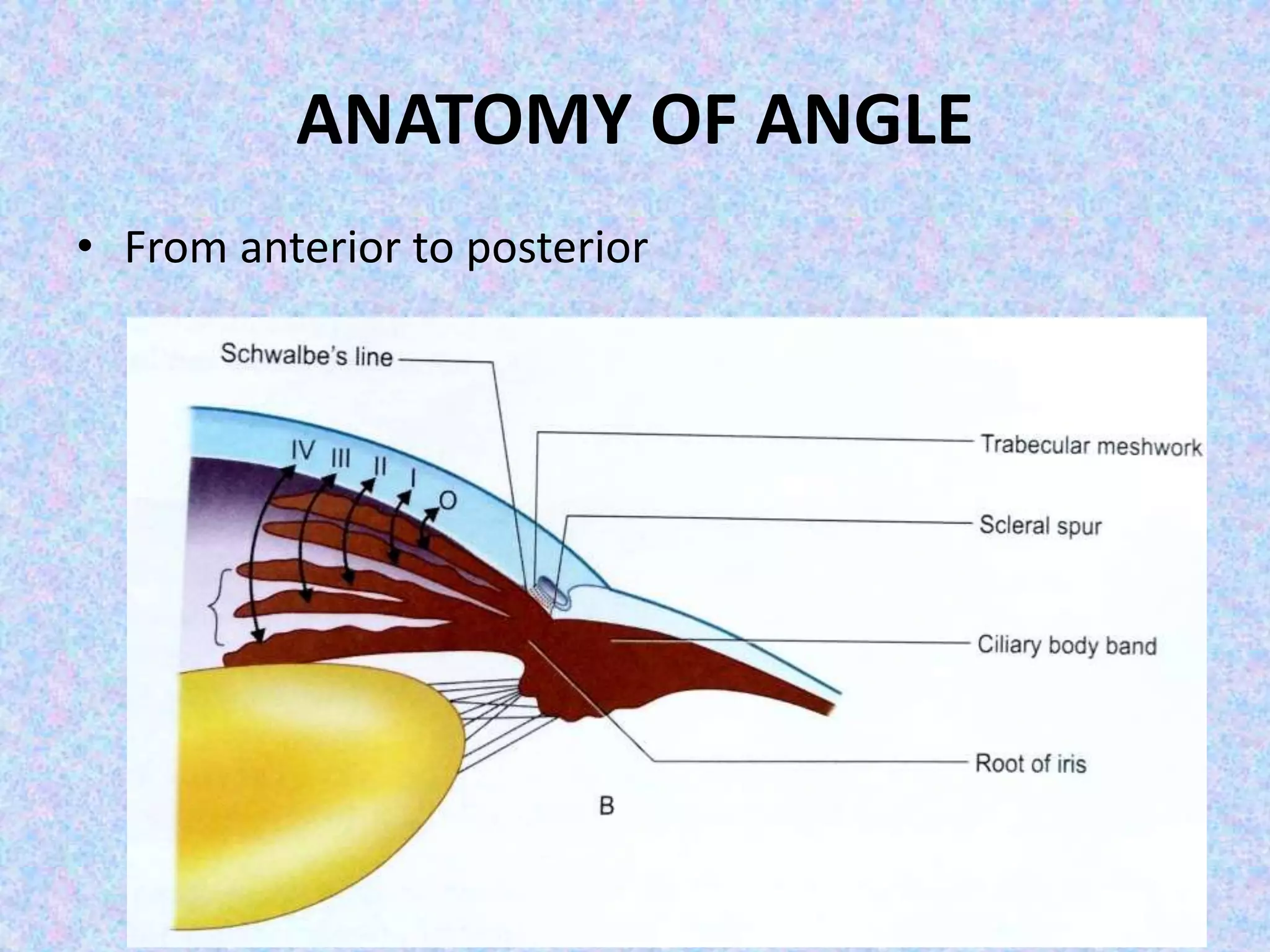

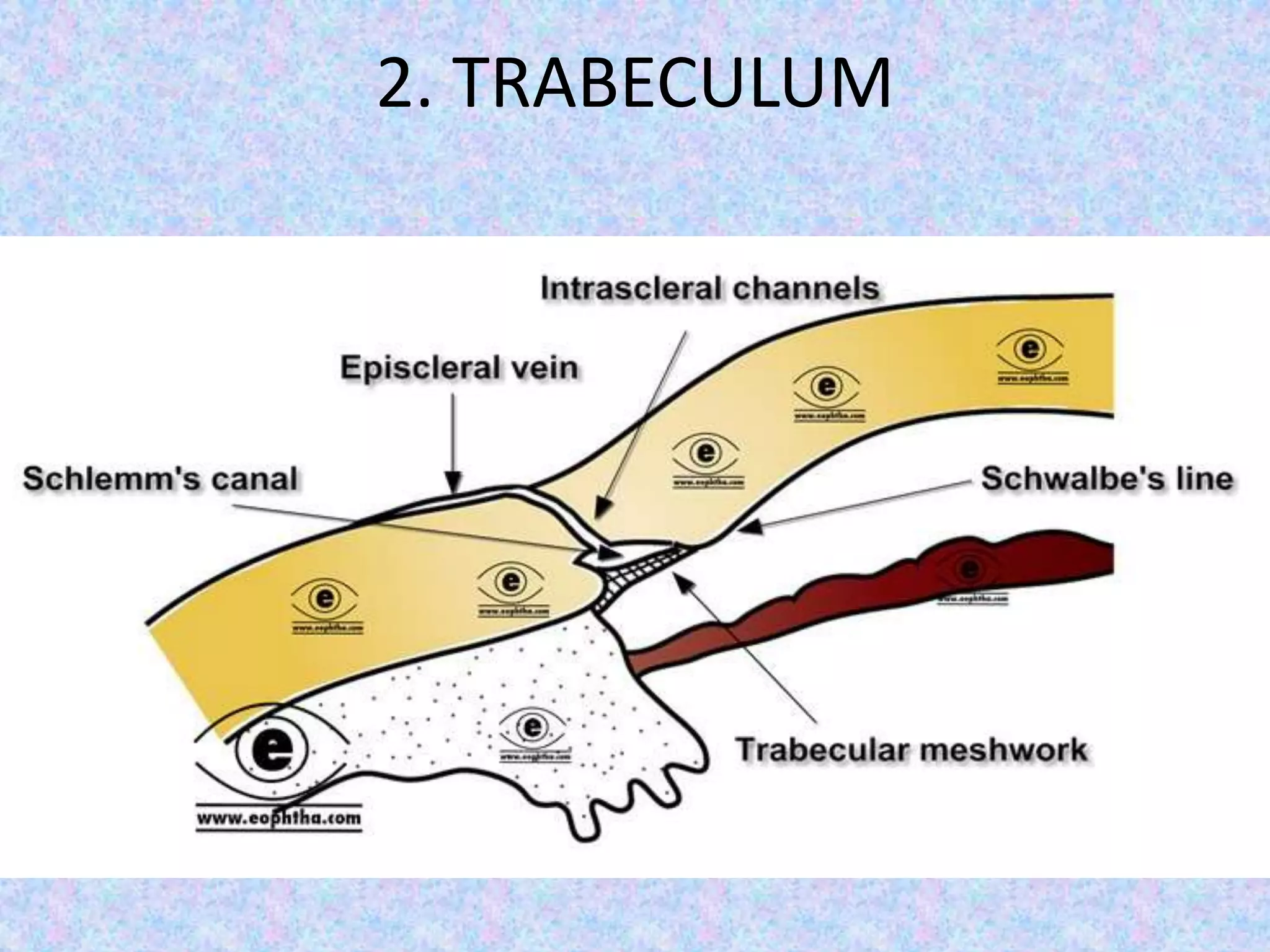
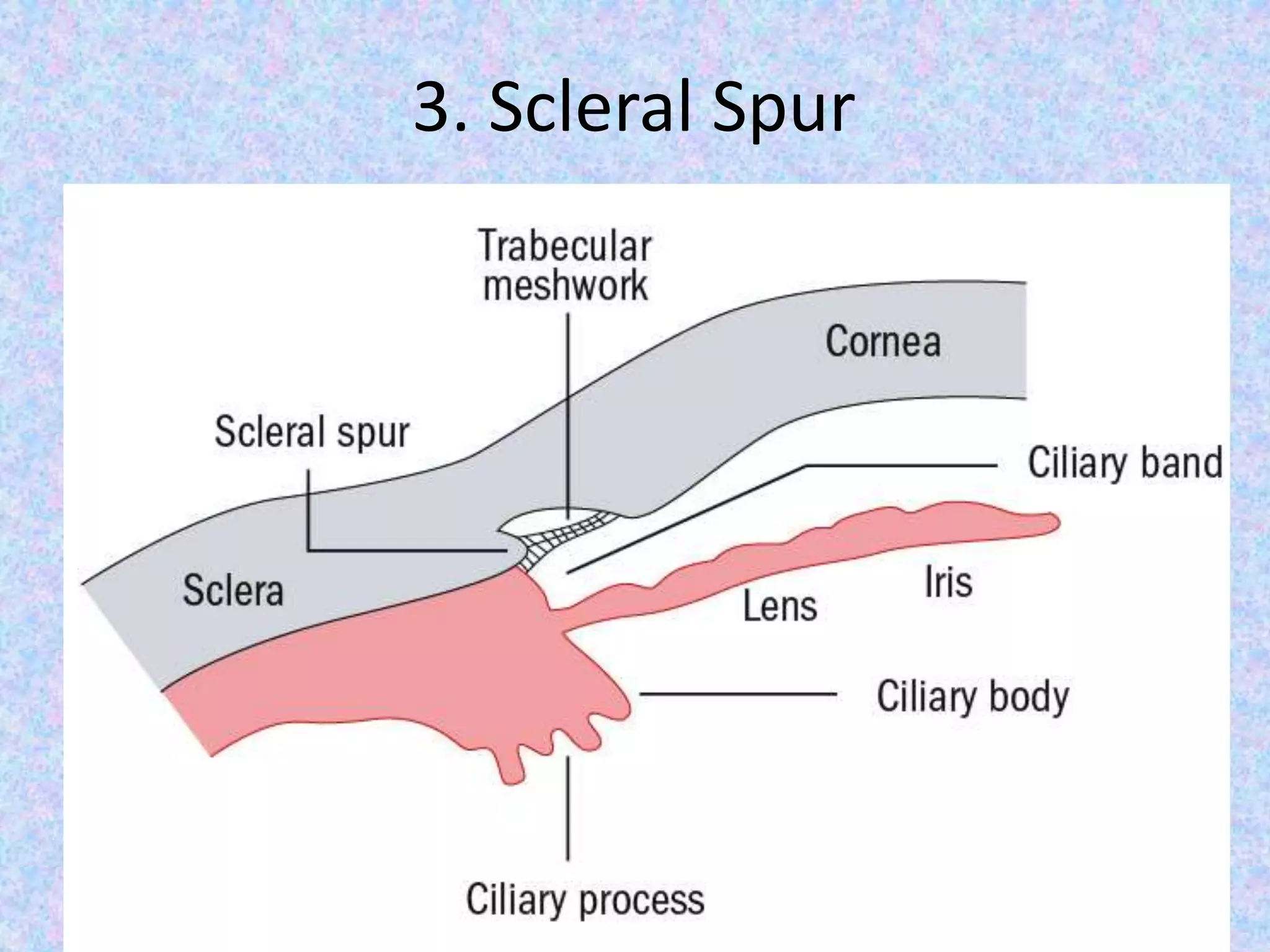
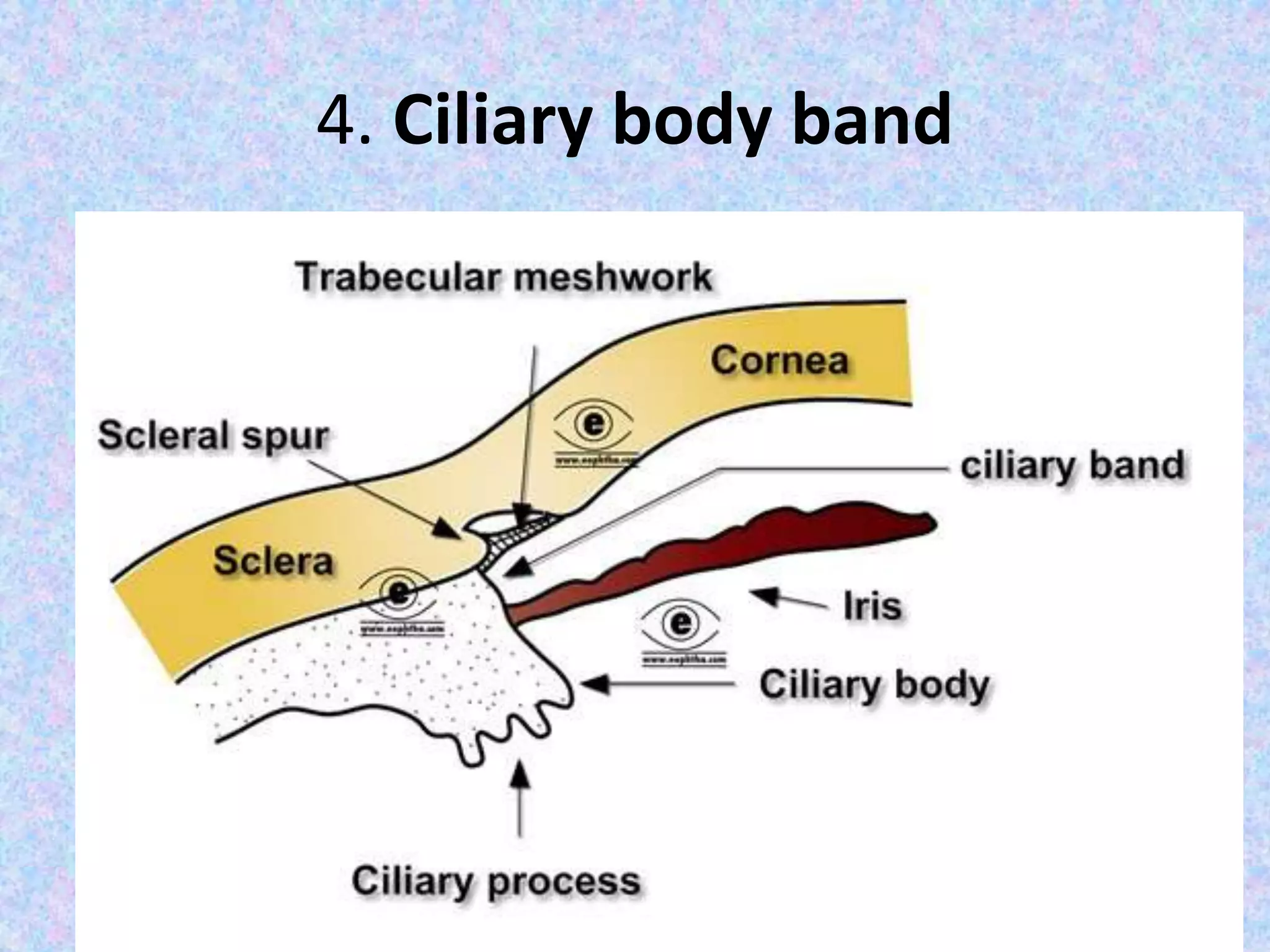





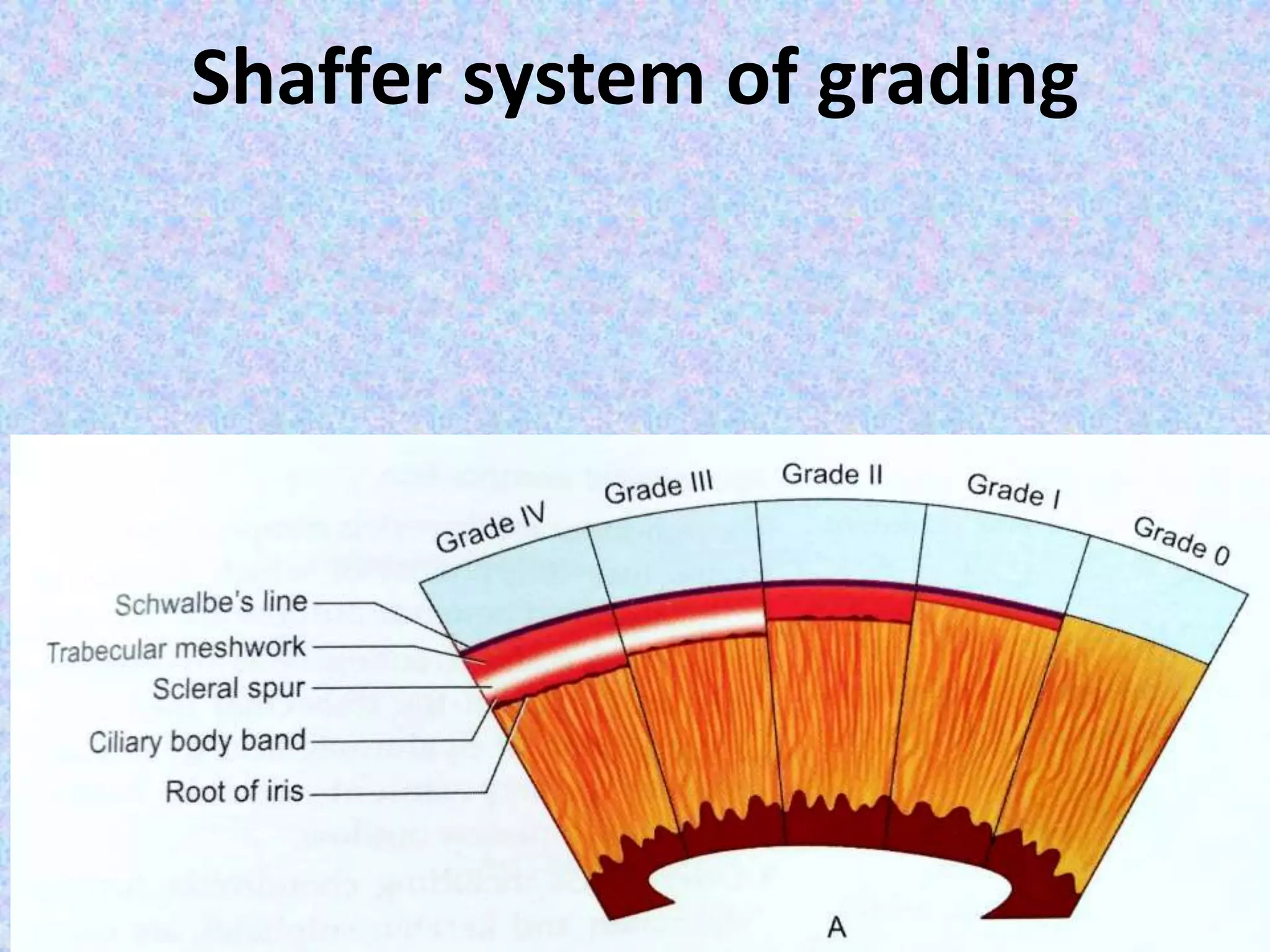
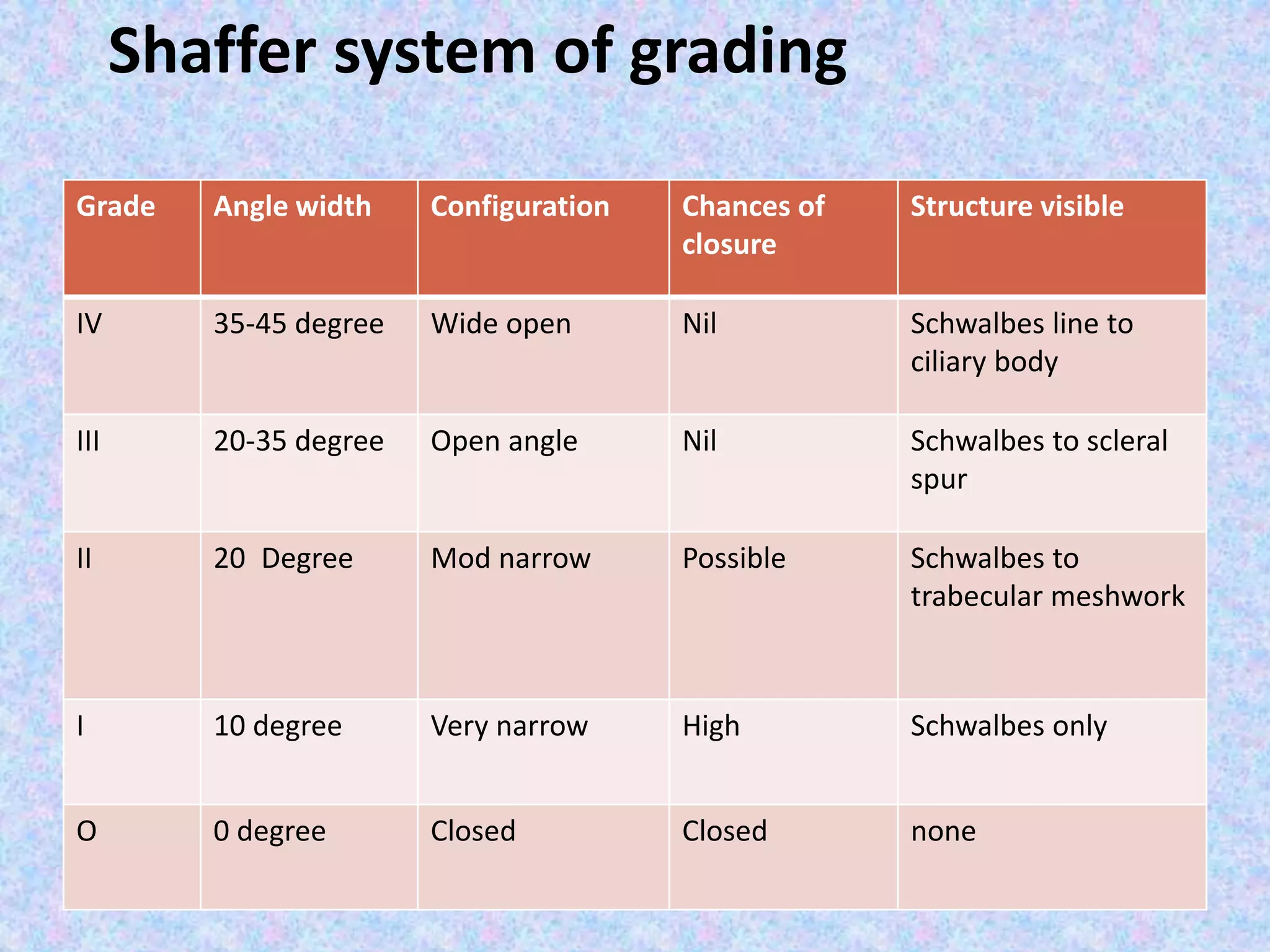
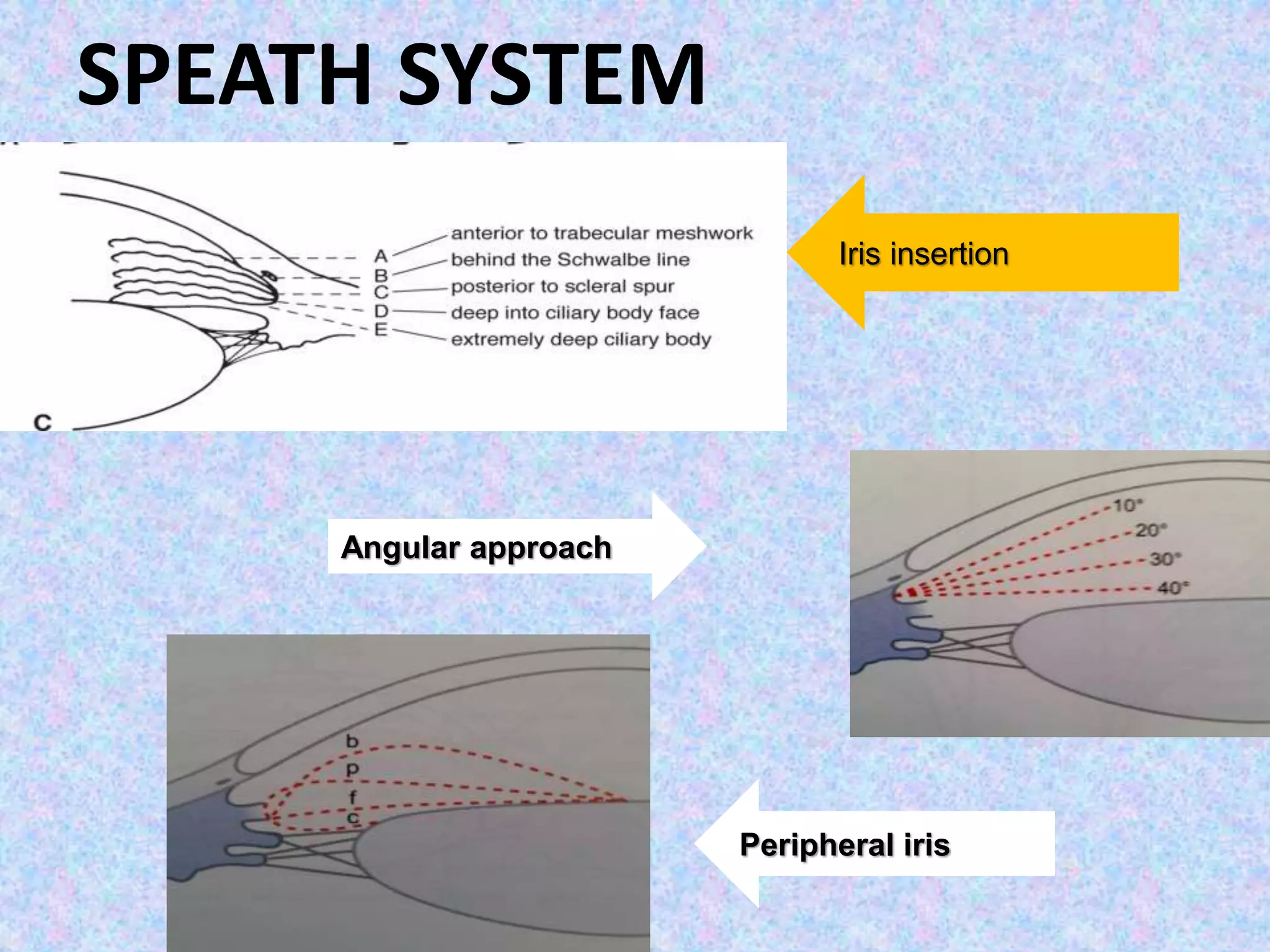
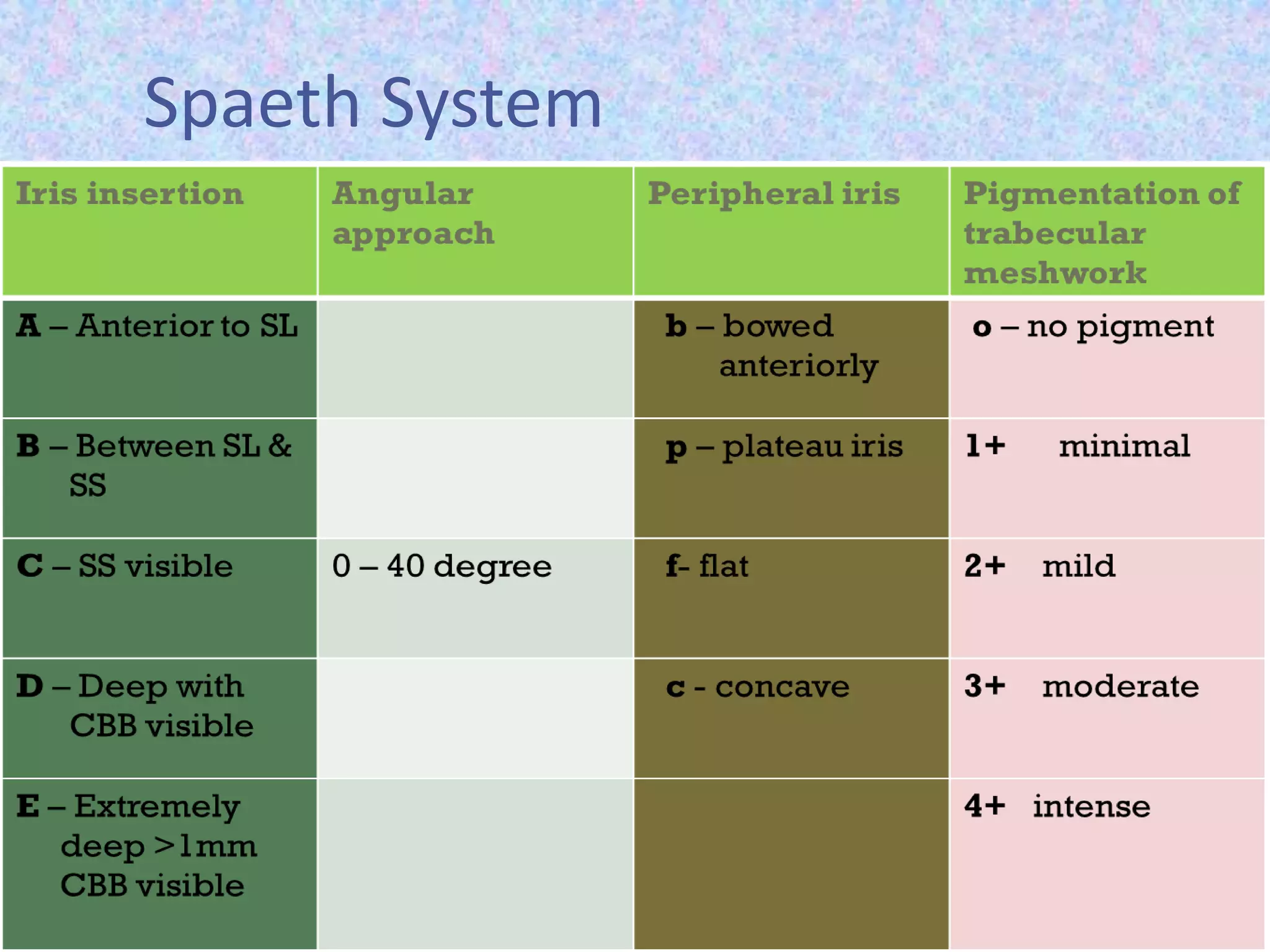
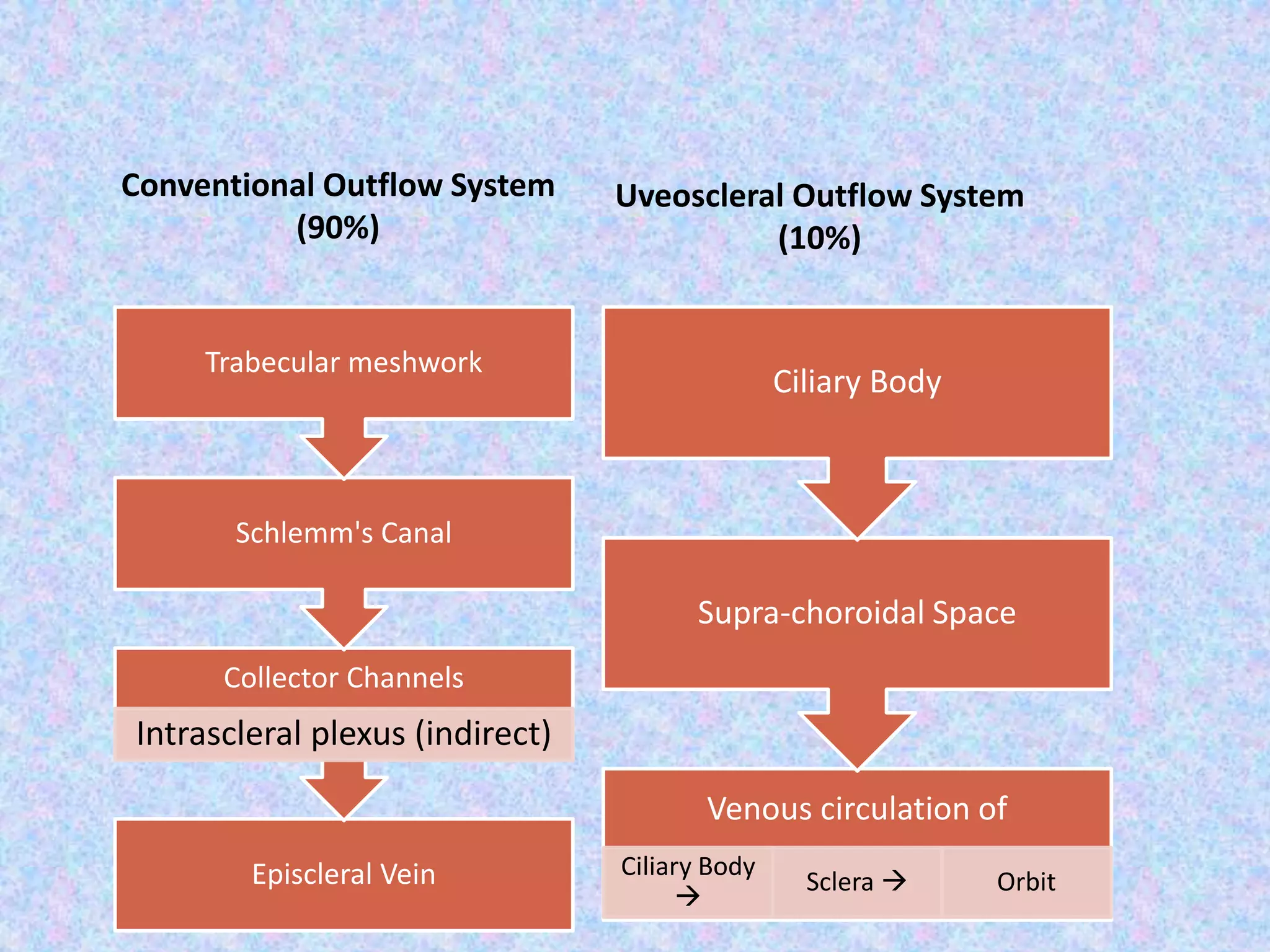

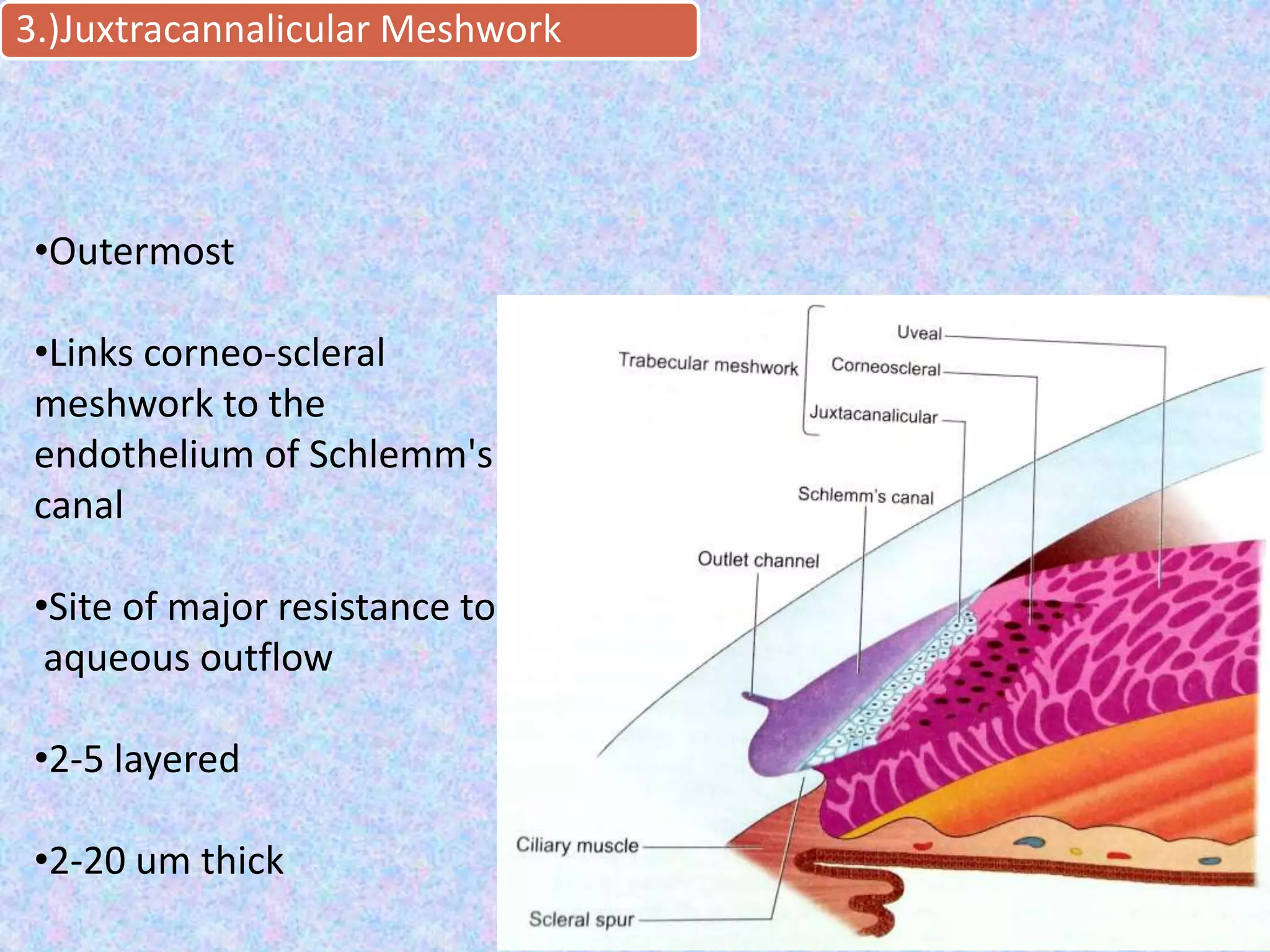




This document discusses the anatomy of the angle structures in the eye and factors that affect intraocular pressure (IOP). It describes the development of the angle structures, including the schlemm's canal, trabecular meshwork, scleral spur, and ciliary body band. It also outlines the assessment of the anterior chamber angle, aqueous drainage system, definition of IOP, and factors that can affect IOP such as age, glaucoma, episcleral venous pressure, and resistance to aqueous outflow. Maintaining the normal range of IOP is important to prevent damage to the optic nerve from conditions like glaucoma.











































































