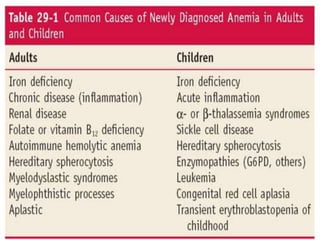
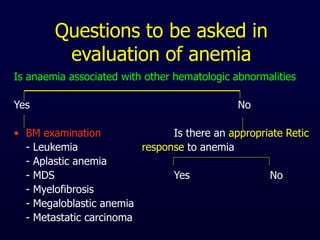
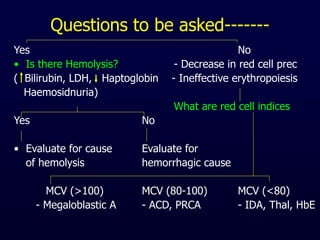
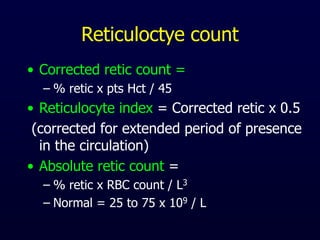
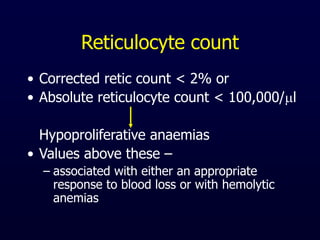
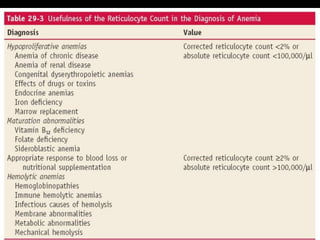
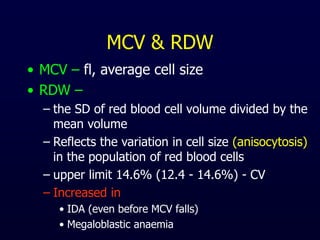
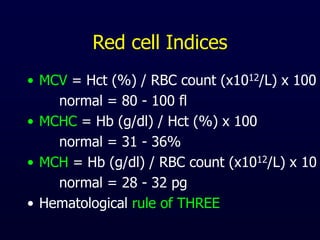
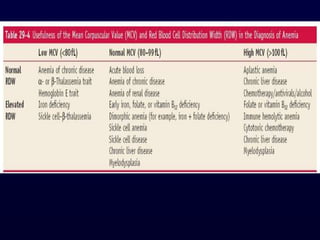
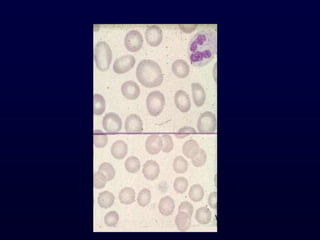
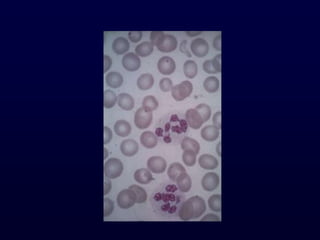
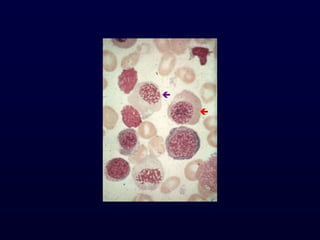
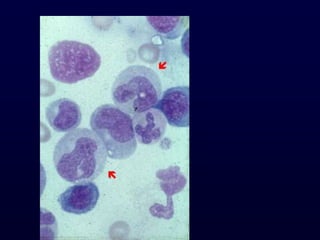
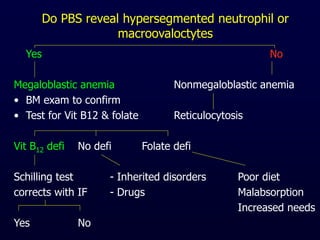
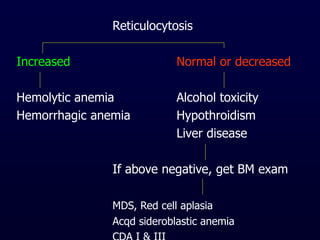
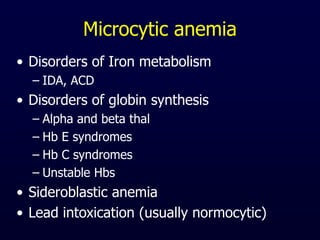
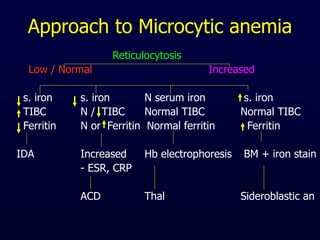
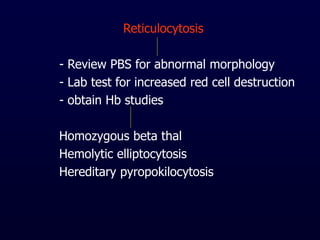
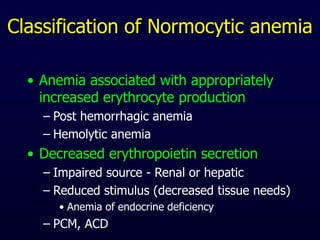
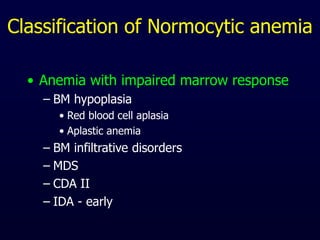
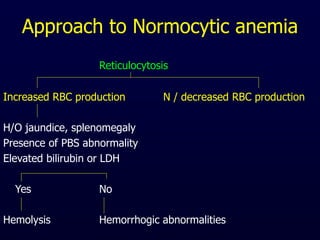
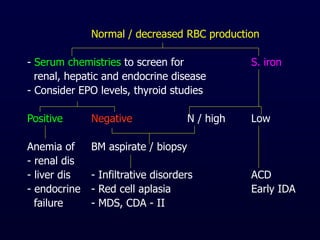
This document provides information on classifying and understanding the pathogenesis of anemia. It discusses definitions of anemia based on hemoglobin levels in adults and children. It also covers evaluating a patient's history for anemia including dietary, medication use, menstrual history, signs and symptoms. The document outlines how to analyze peripheral smear, red blood cell indices, reticulocyte count, and when a bone marrow exam is needed to determine the cause of anemia. It differentiates between macrocytic, microcytic, and normocytic anemias and discusses approach to evaluating each type.






































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









