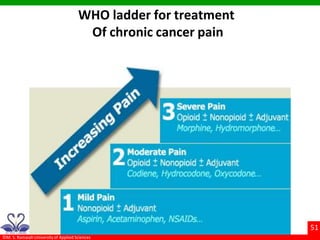
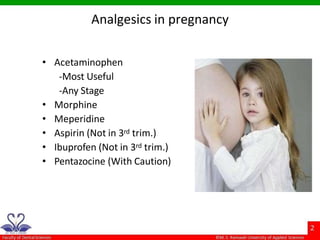
The document provides a comprehensive overview of analgesics and antibiotics used in dentistry, focusing on various classifications and types of analgesics, including NSAIDs and their mechanisms of action. It highlights the pharmacokinetics, adverse effects, and typical uses of these medications, including both topical and systemic applications. Additionally, it addresses the management of chronic pain and treatment considerations for analgesics during pregnancy.


































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


