CONTENTS
Introduction
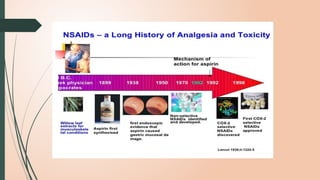
History
Classification
Mechanism of action
Common properties of all NSAIDs
Individual drugs
Choice of NSAIDS
NSAIDS in periodontics
Conclusion
References
4.
PAIN
Definition: Anunpleasant emotional experience usually initiated by a noxious
stimulus and transmitted over a specialized neural network to the central nervous
system where it is interpreted as such- (Monheims)
6.
PAIN CONTROL
• ANALGESICS:A drug that selectively relieves pain by acting in CNS or on peripheral pain
mechanism, without significantly altering consciousness.
ANALGESICS
Opioid analgesics Non opioid analgesics
7.
COMPARED TO OPIODs,NSAIDS ARE :
• Weaker analgesics (except for inflammatory pain)
• Don’t depress CNS
• Don’t produce physical dependence
• No abuse liability
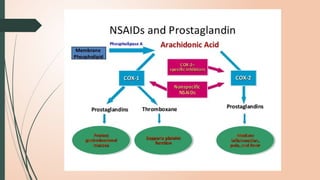
MECHANISM OF ACTION
•NSAIDs – inhibits COX-1 and COX-2 isoforms
• Decrease in PG and Thromboxane synthesis
• Antiinflammatory – reversible inhibition of COX-2
• Aspirin- irreversible inhibition of COX
19.
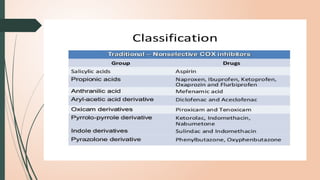
SALICYLATES
Aspirin is acetylsalicylic acid , the prototype converted in the body to
salicylic acid – oldest analgesic .
Other important salicylates – Sulfasalazine , Diflunisal
Natural sources – fruits , vegetables, herbs , spices, nuts and tea
PHARMACOKINETICS
• Salicylates –rapidly absorbed from upper GI tract
• Distributed throughout the tissues and body fluids
• Metabolized – liver- glycine and glucuronide conjugation
• Low doses elimination First order kinetics
• High doses elimination Zero order kinetics
22.
CONTRA INDICATIONS
• Inpatients with peptic ulcer, bleeding tendencies, in children
sufffering from chicken pox or influenza.
• In chronic liver disease: cases of hepatic necrosis have been
reported.
• Should be avoided in those with low cardiac reserve or frank CHF
and in juvenile RA.
• To be avoided in pregnant and breast feeding women.
27.
PROPIONIC ACID DERIVATIVES
•Ibuprofen was the first member of this class to be introduced in
1969.
• Moderate anti-inflammatory effect.
• Better tolerated than Aspirin.
• Can be used in children (doesn’t cause Reye’s syndrome)
• Naproxen being most potent.
29.
• The plasmat1/2 of Ibuprofen is 2hrs .
• Dosage is 400-600mg TDS.
• The plasma t1/2 of Naproxen is 12-16hrs.
• Dosage:- 250mg BD-TDS.
• CONTRAINDICATIONS:-
• Not to be prescribed to pregnant women and peptic ulcer patients
31.
ANTHRANILIC ACID DERIVATIVE(FENAMATE)
Mephenamic acid :
• An analgesic, antipyretic and anti-inflammatory drug, known from
1950s, but has not gained popularity because of lower efficacy.
• Mephanamic acid exerts central as well as peripheral analgesic
actions.
32.
Pharmacokinetics :
• Oralabsorption is slow but almost complete. Highly bound to
plasma proteins .
• plasma t ½ is 2-4 hours.
• Dose: 250-500mg TDS
Uses :
• Analgesic in muscle, joint and soft tissue pain, dsymenorrohea,
rheumatoid and osteoarthritis.
• Antipyretic
• Weak anti-inflammatory effect
33.
Adverse effects :
•Epigastric distress, skin rashes, dizziness and other CNS
manifestations.
• Haemolytic anaemia is rare but serious complication.
34.
ARYL-ACETIC ACID DERIVATIVES
DICLOFENACSODIUM:
• Potent atnti-inflammatory effect
• Gets concentrated in synovial fluid, hence preferred in
inflammatory conditions of joint
• Incidence of hepatotoxicity is more
• Diclofenac + misoprostol – reduces GI irritation and peptic ulcer
35.
USES:-
• Diclofenac isthe most extensively used NSAID; employed in
Rheumatoid and Osteo Arthritis, toothache, ankylosing spondylitis,
dysmenorrhoea, post traumatic and post inflammatory conditions-
affords quick relief of pain and wound edema.
• Dosage:-
• 50mg BD, 1OOmg OD
36.
Pharmacokinetics
• It iswell absorbed orally, 99% protein bound, metabolized and
excreted both in urine and bile.
• The plasma t1⁄2 is ~2 hours. Due to good tissue penetrability,
concentration in joints and other sites of inflammation is maintained
for longer period extending the therapeutic effect
Adverse effects :
• Epigastric pain, nausea, headache, dizziness, rashes.
• Gastric ulceration and bleeding are less common.
37.
OXICAM DERIVATIVE
PIROXICAM
• Itis long lasting action with potent anti inflammatory and good
analgesic action.
• It is a reversible inhibitor of COX, lowers PG synthesis and inhibits
platelet aggregation.
• In addition, it decreases the production of IgM Rheumatoid Factor
and reduces leucocyte chemotaxis-thus inhibits inflammation in
diverse ways.
• It is 99%plasma protein bound , plasma t1/2 is nearly 2 days.
• Dose is 20mg BD for two days followed by 20 mg OD.
38.
Uses:-
• Short termanalgesic as well as long term anti inflammatory in
Rheumatoid and OsteoArthritis, Ankylosing Spondylitis, Acute Gout,
musculoskeletal injuries and in dentistry.
Adverse effects:-
• Heart burn
• Rashes
• Nausea
• Edema
39.
PYRROLE DERIVATIVE
KETOROLAC:
• ThisNSAID has potent analgesic , efficacy almost equal to morphoine
• Relieves pain without causing respiratory depression, hypotension and
drug dependence.
• Used in renal colic, postoperative and metastatic cancer pain
40.
Pharmacokinetics:
• Ketorolac israpidly absorbed after oral and i.m. administration.
• It is highly plasma protein bound and 60% excreted unchanged in
urine.
• plasma t1⁄2 is 5–7 hours.
41.
Adverse effects :
•Nausea, abdominal pain, ulceration, loose stools, drowsiness,
headache, dizziness, nervousness, pruritus, pain at injection site, rise
in serum transaminase and fluid retention have been noted.
Uses:
• Ketorolac is frequently used in postoperative, dental and acute
musculoskeletal pain: 15– 30 mg i.m. or i.v. every 4–6 hours (max. 90
mg/ day).
• It may also be used for renal colic, migraine and pain due to bony
metastasis.
42.
INDOLE DERIVATIVE:
Indomethacin:-
• Thisindole acetic acid derivative is a potent anti inflammatory drug
with prompt antipyretic action.
• Very effective in ankylosing spondylitis and psoriatic arthritis
• Side effects- GI, CNS
• Contraindicated in epileptic, psychiatric patients and drivers.
43.
Pharmacokinetics:
• Indomethacin iswell absorbed orally.
• It is 90% bound to plasma proteins, partly metabolized in liver to inactive products
and excreted by kidney.
• Plasma t1⁄2 is 2–5 hours.
Adverse effects:
• A high incidence (up to 50%) of gastrointestinal and CNS side effect is produced.
• Gastric irritation, nausea, anorexia, gastric bleeding and diarrhoea are prominent.
• Frontal headache (very common), dizziness, ataxia, mental confusion,
hallucination, depression and psychosis can occur.
Leukopenia, rashes and other hypersensitivity reactions are also reported.
• Increased risk of bleeding due to decreased platelet aggregability.
44.
Uses:
• Indomethacin isused as a reserve drug in conditions requiring potent
anti inflammatory action like ankylosing spondylitis, , psoriatic arthritis
and acute gout or rheumatoid arthritis that are not responding to
better tolerated NSAIDs.
• Malignancy associated fever.
• medical closure of patent ductus arteriosus.
45.
PYRAZOLONES
• Antipyrine (phenazone)and amidopyrine (aminopyrine) were introduced in
1884 as antipyretic and analgesic.
• Phenylbutazone was introduced in 1949 and soon its active metabolite
oxyphenbutazone was also marketed.
• These two are potent anti inflammatory drugs, inhibit COX, but have slow
onset, weak analgesic and antipyretic action.
46.
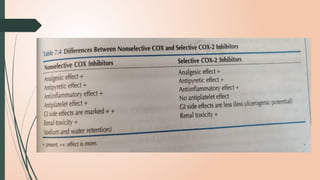
PREFERENTIAL COX-2 INHIBITORS
NIMESULIDE:
•It is a week inhibitor of PG synthesis and indicate relative cox 2
selectively.
• Used in sports injury , sinusitis, dental surgery, post op pain , fever.
• Absorbed orally,99% plasma protein bound.
• T1/2 of 2-5hrs
47.
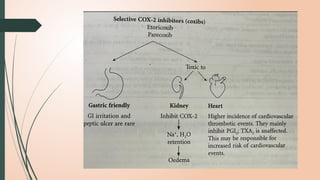
SELECTIVE COX-2 INHIBITORS(Coxibs)
• The theoretical advantage of inhibiting COX-2 without affecting
COX-1 function, some highly selective COX-2 inhibitors are
introduced.
• They cause less gastric mucosal damage; occurrence of peptic ulcer
and ulcer bleeds is clearly lower than with traditional NSAIDs.
• They do not depress TXA2 production by platelets (COX-1
dependent); do not inhibit platelet aggregation or prolong bleeding
time, but reduce PGI2 production by vascular endothelium.
49.
• Currently, 3selective COX-2 inhibitors (also called coxibs) Celecoxib,
Etoricoxib and Parecoxib are available in India.
• Rofecoxib and Valdecoxib were withdrawn within few years of marketing
for increasing cardiovascular (CV) risk.
• It has been concluded that selective COX-2 inhibitors should be used only
in patients at high risk of peptic ulcer, perforation or bleeds.
• If selected, they should be administered in the lowest dose for the shortest
period of time.
50.
CELECOXIB:
• It exertsanti inflammatory, analgesic and antipyretic actions with low
ulcerogenic potential.
• Comparative trials in rheumatoid arthritis have found it to be as effective as
naproxen or diclofenac, without affecting COX-1 activity in gastro duodenal
mucosa.
Pharmacokinetics:
• Celecoxib is slowly absorbed,
• 97% plasma protein bound . t1⁄2 of ~10 hours.
Dose:
• It is approved for use in osteo- and rheumatoid arthritis in a dose of 100–200 mg
BD.
52.
Analgesic –antipyretics withpoor anti-inflammatory effe
• PARACETAMOL:
• (Acetaminophen) the de ethylated active metabolite of phenacetin, was introduced in 1950.
• ACTIONS:
• The central analgesic action of paracetamol is like aspirin, i.e. it raises pain threshold, but has
weak peripheral anti inflammatory component.
• Analgesic action of aspirin and paracetamol is additive. Paracetamol is a good and promptly
acting antipyretic.
• Paracetamol has negligible anti inflammatory action. It is a poor inhibitor of PG synthesis in
peripheral tissues, but more active on COX in the brain.
53.
PHARMACOKINETICS:
• Paracetamol iswell absorbed orally, only about 1/4th is protein bound in plasma and it is
uniformly distributed in the body.
• Metabolism occurs mainly by conjugation with glucuronic acid and sulfate: conjugates are
excreted rapidly in urine.
• Plasma t1⁄2 is 2–3 hours. Effects after an oral dose last for 3–5 hours.
USES
• Paracetamol is one of the most commonly used ‘over-the-counter’ analgesic for headache,
mild migraine, musculoskeletal pain, dysmenorrhoea, etc. but is relatively ineffective when
inflammation is prominent as in rheumatoid arthritis.
• Paracetamol is recommended as first choice analgesic for osteoarthritis by many professional
bodies.
• In contrast to Aspirin, Paracetamol does not stimulate respiration or affect acid-base balance;
does not increase cellular metabolism. It has no effects on CVS, platelet function , gastric
mucosa.
MECHANISM OF TOXICITYAND TREATMENT
• Toxic metabolite – detoxified by conjugation with glutathione and gets
eliminated
• High doses- depletion of glutathione
• Toxic metabolites- proteins- liver and kidney- necrosis
• Alcoholics and premature infants – hepatotoxicity
• Oral methionine replenishes glutathione store of liver and protects the liver
• Activated charcoal – decrease the absorption of paracetamol from gut
56.
GUIDELINES FOR USAGEOF NSAIDS
• Mild-to-moderate pain with little inflammation: paracetamol or low-dose ibuprofen.
• Postoperative or similar acute but short- lasting pain: ketorolac, a propionic acid
derivative.
• Exacerbation of rheumatoid arthritis, ankylosing spondylitis, acute gout, acute
rheumatic fever: naproxen, piroxicam, indomethacin, high dose aspirin.
• Gastric intolerance to traditional NSAIDs or predisposed patients: a selective COX-2
inhibitor or paracetamol.
• Patients with history of asthma or anaphylactoid reaction to Aspirin or other NSAIDs:
Nimesulide, COX-2 inhibitor.
• Paediatric patients: only paracetamol, aspirin, ibuprofen and naproxen have been
adequately evaluated in children — should be preferred in them. Due to risk of
Reye’s syndrome, aspirin should be avoided.
57.
HOST MODULATION BYNSAIDS
• Goldhaber and coworkers examined whether prostaglandins might be
responsible in part for the gingival-tissue extract mediated bone resorption. They
were studying by adding indomethacin to the culture media, as an inhibitor of
cyclooxygenase.
• The prostaglandin production blocked by indomethacin decreased the bone
resorption in tissue culture by up to 50% .
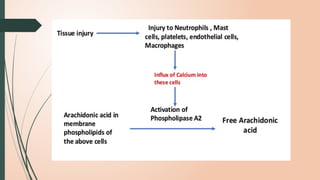
• Free arachidonic acid (AA) is produced in the hosts when phospholipase A2
acts on the phospholipids present in plasma membranes of the cells which can
then be metabolized to produce prostaglandins via the cyclooxygenase (COX)
pathway as well as leukotrienes via the lipoxygenase (LOX) pathway.
58.
• Non steroidalanti inflammatory (NSAIDs) drugs block the activity of both
‐ ‐
cyclooxygenase isozymes (COX- 1 and -2) and many authors have demonstrated
the role of NSAIDs like flurbiprofen, indomethacin, and naproxen, in inhibiting
gingivitis and progression of periodontitis
• Since NSAIDs are lipophilic and are well absorbed into gingival tissues, its topical
application is possible.
• NSAIDs that have been evaluated for topical administration include ketorolac,
tromethamine rinse and S-ketoprofen dentifrice, piroxicam and meclofenamic
acid in inhibiting gingivitis and progression of periodontitis.
59.
• Waite etal (1981) demonstrated that subjects taking several types of NSAIDs,
which included phenylbutazone, indomethacin, aspirin, a combination of
phenylbutazone and indomethacin, as well as other medications, had less
gingival inflammation and shallower pocket depths than a control population
not taking medications.
• In studying the NSAID ibuprofen and its effect on periodontal disease, Williams
et al. (1988) demonstrated that high (4 mg/kg) and low (0.4 mg/kg) doses of
ibuprofen in both sustained release and normal release formulations resulted
in reduction in the rate of bone loss.
THE EFFECT OF NSAIDS ON PERIODONTAL DISEASE
REFERENCES
• Tara VShanbhag, Pharmacology for dentistry
• Tripati KD. Non steroidal anti inflammatory drugs. In: Essentials of medical pharmacology: 7, Jaypee
publishers; 2013: 192-205.
• General physiology book sembulingam.
• Caranza text book .8th edition.
• Tripati KD. Prostaglandins, leukotrienes and platelet activating factor. In: Essentials of medical
pharmacology: 7, Jaypee publishers; 2013: 181-191.
• Sembulingam for physiologyDewhirst. F. E.: 6-Keto-Prostaglandin El Stimulated Bone Resorption in Organ
Culture. Calcif. Tissue Int. 1984; 36:380-383.
• Heasman, P. A. and R. A. Seymour. The Effect of a Systemically-administered Nonsteroidal Anti
inflammatory Drug (Flurbiprofen) on Experimental Gingivitis in Humans. J Clin.Periodontol 1989; 16:551- 556.
Editor's Notes
#3 Chewing of willow bark for variety of ailments
Mclagan 1876- extracted a portion of willow bark called salicia
1899- german pharmaceutical company – bayer – developed acetyl salicylic acid- Aspirina
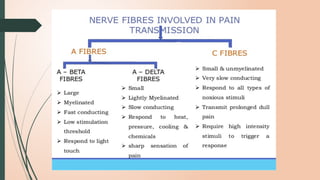
#5 Information about touch and pain –trnsmtd- brain n spinal cord- primary afferent axons.
Nerve fibres- connctd to df types of receptors on skin , muscles and internal organs.
PAA-df diameters and divided into df groups based on their size and myelination
In order of decreasing size- Aalpha, Abeta, Adelta and C fibres.
A AL,B, D are myelinated . C unM
C FFIBRES- Condctn rate- 0.5 to 2m/s. A delta- 5-30m/s ABETA– 35 to 120 m/s
Stimuli- mechanical, thermal or metabolic smallest and slowest of myelinated axons
Pain produced- slw, burning and long lasting stimuli- either mechanical or temperature
Neurotransmitter in dorsal horn- glutamate along with substance P pain- sharp bright pain
neurotransmitter –dorsal horn- glutamate
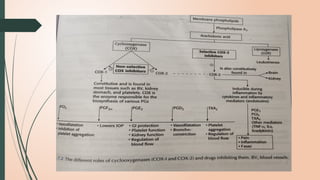
#11 PG-product of long chain fatty acids
AA-precursor for bioS of all PG
COX-enzyme
Main PG in humans- PGE2, PGF2ALPHA , ProstaCylin
When LOX acts on AA –Leukotrines
COX1 – participates in various physiological functions such as protection of gastric mucosa, homeostatis, regulation of cell division
COX2 is induced during inflmn by cytokines and endotoxins
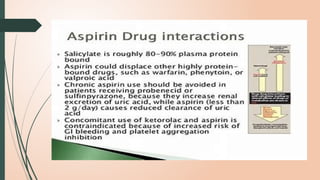
#16 The antithrombotic effect of aspirin results largely from irreversible inhibition of the cyclooxygenase-1 enzyme in platelets, leading to impaired platelet aggregation and activation [139, 140]. Aspirin therapy could reduce recurrent ischemic events, but also could put the patient at risk of an intracranial hemorrhage.
#17 OTHER USES
colon and rectal cancer
Alzheimer's disease- aspirin- reduces the risk and retards the onset
Radiation induced diarrhoea
Analgesic effect- peripheral inhibition of PG prodn
They increase pain threshold- subcortical site
Cause pain redn- without causing sedation, tolerance or drug dependence.
Thermoregulatory centre- hypothalamus
Fever- disturbance in the thermostat
Nsaid- reset the hypothalamic thermostat - reduce the elevated body temp
Cutaneous vasodilation and sweating
Antipyretic- inhibition PG in hypothalamus
Donot alter the disease progression. Symptomatic relief
Aspirin
Reduces fever, swellimg, joint pain
Paracetamol-mild cases
Topical agents – methyl salicylate, diclofenac gel
Circulating blood clot- gets stuck – causes obstruction
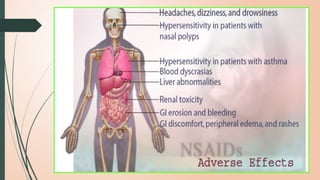
#18 Skin lesion
Drug interaction
Nausea , vomiting, ulcers acute gastritis, GI bleeding
After food
Proton pump inhibitors or H2 blockers with NSAIDs
Selective COX2 inhibitors
ASPIRIN
Skin rashes, rhinitis, bronchospasm, angioneurotic edema, anaphylactoid rxn
Bronchospasm(aspirin induced asthma) – increased prodn of leukotrienes
Incidence is high—asthma, nasal polyps, recurrent rhinitis
Prolonged use of salicylates– interferes with the action of vit k in the liver – decreased synthesis of clotting factors – bleeding
Salicylates- children with viral infection– encephalopathy and hepatic damage with fatty infiltration
Delay onset of labour, increases chnces of pp hemorrhage
New borne- premature closure of ductus arteriosus9bv cnctg PA to AORTA)
Prolonged use- renal damage– rreversible
#20 The Analgesic effect is mainly due to obtunding of peripheral pain receptors & prevention of PG-mediated sensitizatio of nerve endings.
Antipyretic- resets the Hypothalamic thermostat & Rapidly reduces fever by promoting heat loss but does not reduce heat production
Anti inflammatory at high doses(3-5g/day or 100mg/kg/day)
Suppress signs ans symptoms of inflmn such as pain, trendernessselling, vasodilation and leukocyte infiltration
AI is bcz. They also inhibit mediators of inflmn histamine, bradykinin,serotonin etc.
Irriversibly inhibits TXA2 synthesis and produces antiplatelet effect for 8-10
High doses- inhibits both PGI2 and TXA2 . So beneficial effects of PGI2 is lost.
Withdrawn 1 week prior top surgery to reduce the risk of bl;eeding
Prolonged use– cause sodium and water retention
Precipitates CCF in patients with low cardiac reserve
Decrease the effect of antihypertensive drugs
#21 The plasma t1/2 of Aspirin as such is 15-20min, but taken together with that of salicylic acid, is 3-5hrs.
However, metabolic processes get saturated over the therapeutic range; t1/2 of anti inflammatory doses may be 8-12hrs.
After this, an inc in salicylate dosage – increases its plasma conc disproportionately – severe toxicirty
Alkalinization of urine –increases the rate of excretion of salicylates
#23 DOSAGE
PROPHYLACTIC DOSE- 75-100MG once a day
Adult dose
The usual single dosage is 300-600 mg (1-2 tablets). It should not exceed 1 gr. This dose can be administered 3 to 4 times a day at 4 -8 hour intervals. The maximum dose per day should be lower than 3 grams.
Rhe4matic fever—80 mg/kg
#29 Reduces the blood flow to babys kidneys and other structures
#60 NSAIDs are the mainstay for management of acute dental pain. The cause and nature of pain along with consideration of the risk factors in the patient govern the selection of analgesic. Thus No Single drug is superior to all others for every patient.