Download to read offline




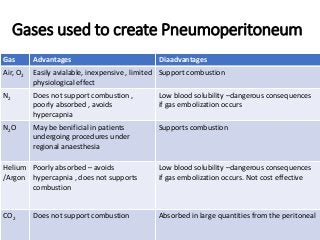
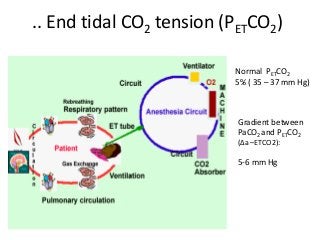
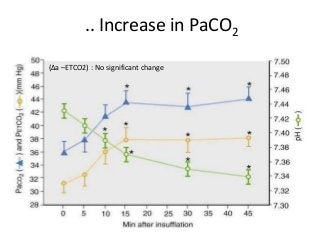
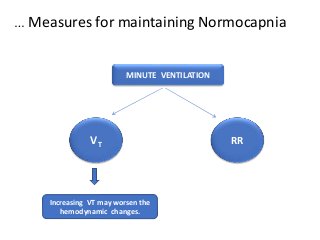

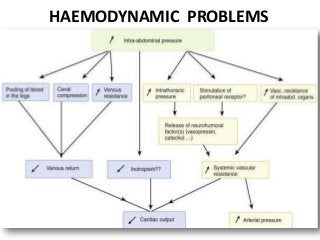
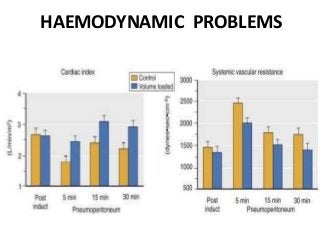
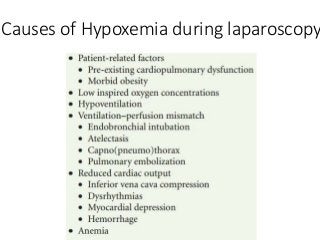
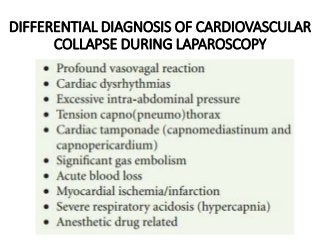
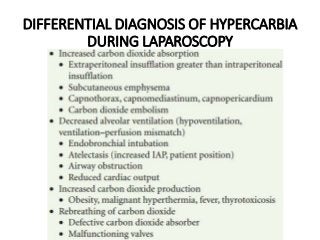
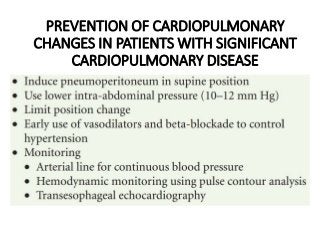


The document discusses anaesthetic considerations for laparoscopic cholecystectomy, highlighting the advantages of minimally invasive surgery such as reduced postoperative pain and complications. It details the physiological changes induced by pneumoperitoneum and positioning, as well as the associated respiratory and hemodynamic complications. Additionally, it outlines preoperative assessments, intraoperative management strategies, and postoperative care recommendations to mitigate risks during the procedure.











































![shalini laparo [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shalinilaproautosaved-231107054900-e5005f6e-thumbnail.jpg?width=640&height=640&fit=bounds)











































