Download to read offline





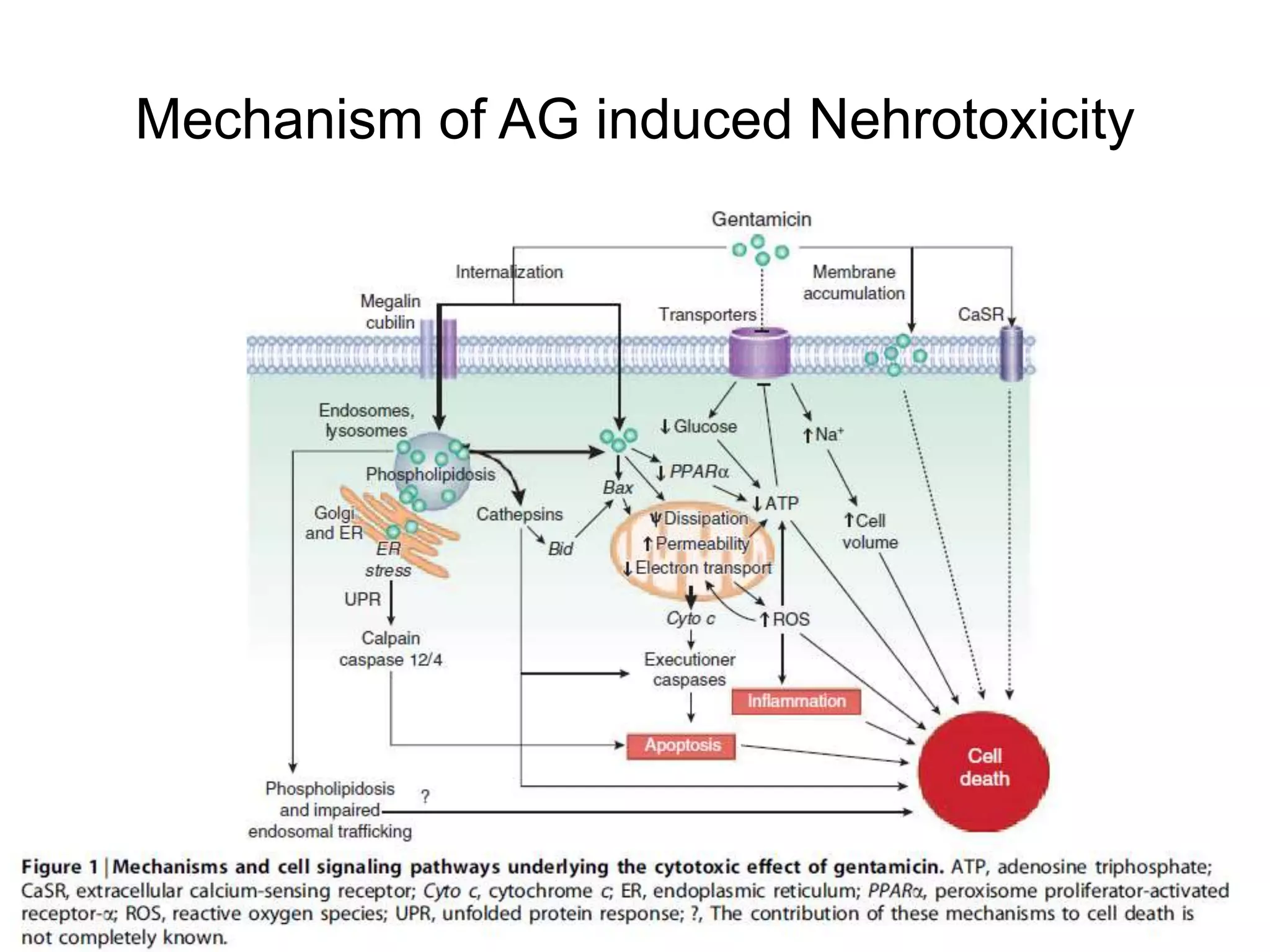











Aminoglycoside antibiotics can cause acute kidney injury (AKI) in 10-15% of patients through nephrotoxic mechanisms. Risk factors include pre-existing kidney dysfunction, hypokalemia, and reduced effective arterial volume. AKI occurs 5-7 days after treatment and is usually non-oliguric and mild, though it can be severe. Prevention focuses on selecting less toxic aminoglycosides, correcting electrolyte abnormalities, limiting duration of therapy, and minimizing other nephrotoxins. While various compounds have shown promise in preventing aminoglycoside-induced nephrotoxicity, none are used clinically.




















































































