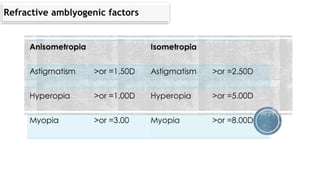
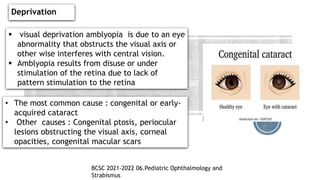
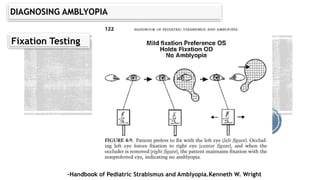
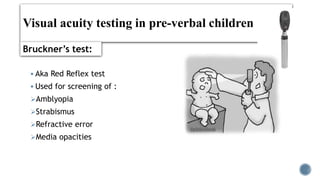
The document discusses amblyopia, including its definition, causes, types, visual development milestones, diagnosis, and abnormalities found in amblyopic eyes. It provides details on epidemiology, pathophysiology, classification, and visual characteristics of amblyopia such as crowding phenomenon, eccentric fixation, and reduced contrast sensitivity. The document also outlines methods for diagnosing amblyopia in pre-verbal children through tests of fixation, red reflex, and induced tropia.