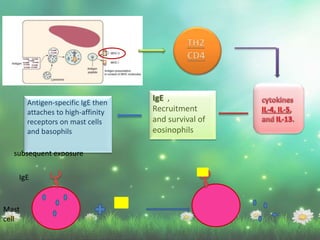
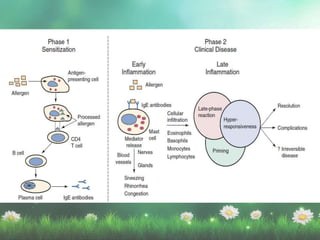
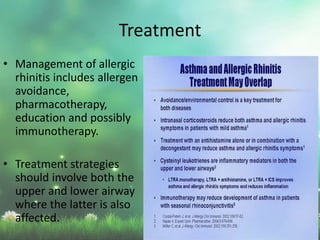
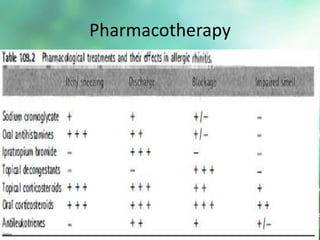
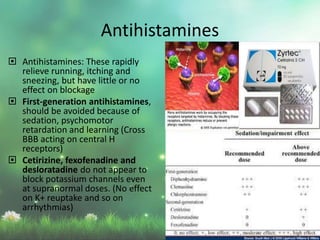
Allergic rhinitis is a type I hypersensitivity reaction mediated by IgE antibodies. It has a prevalence of 10-20% in the US and is characterized by symptoms like sneezing, rhinorrhea, nasal congestion and pruritus. Risk factors include family history of atopy, environmental exposures, and lifestyle factors. Treatment involves allergen avoidance, pharmacotherapy with antihistamines, intranasal corticosteroids, leukotriene receptor antagonists and immunotherapy for selected patients.