Downloaded 15 times


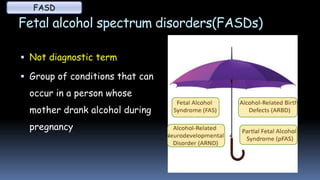


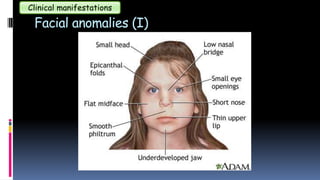



1) Alcohol use during pregnancy can cause fetal alcohol spectrum disorders (FASDs), which include fetal alcohol syndrome (FAS) and other conditions involving physical abnormalities, developmental delays, and cognitive impairments. 2) Clinical manifestations of FASDs can include facial anomalies, growth retardation, central nervous system anomalies affecting both structure and function of the brain, and other issues affecting organs like the heart, kidneys and skeleton. 3) FASDs are preventable if a woman does not consume any alcohol during pregnancy, as there is no known safe amount of alcohol use when a woman is pregnant.

















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



