Download to read offline



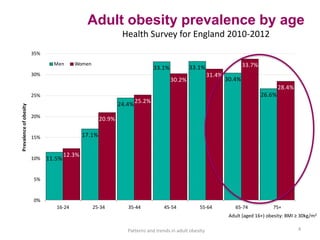
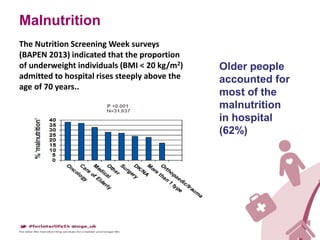

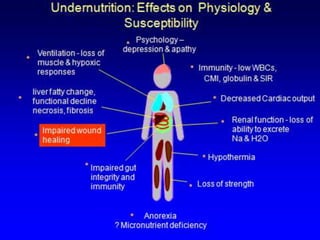





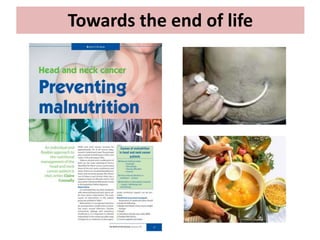


This document discusses nutrition and well-being in later life. It notes that malnutrition increases sharply after age 70 and older adults account for most malnutrition in hospitals. Good nutrition can help manage chronic disease and weight, while undernutrition increases disease risk and negatively impacts mood and quality of life. Specific nutrients like vitamins and fatty acids affect well-being and cognition. Towards the end of life, the document questions whether individual needs and preferences of older adults are adequately considered regarding food, which can impact dignity, anxiety and quality of life.